Join our clinical trials
This could be your breakthrough. Let's do this! Bonus! It's fast and Free!
The Neuro Recursion Institute (NRI) studies the neurological feedback loops that drive chronic anxiety and motor urgency in neurodivergent populations. At the core of many neurodivergent conditions, such as, but not limited to Tourette Syndrome, Stuttering, ADHD, OCD, and many phobias is a phenomenon of pathological signaling within the Cortico-Striato-Thalamo-Cortical (CSTC) circuits. When these inhibitory filters fail, a "premonitory urge" triggers a recursive loop where the brain's output constantly re-feeds as a new, amplified input. Our protocol focuses on interrupting these self-perpetuating cycles, providing patients with a neurological "off-ramp" that de-escalates the recursive activity before it manifests as a physical tic, seizure, or a panic response.Research indicates that neurodivergence often involves a distinct processing of dopamine and sensory information within the basal ganglia, leading to what is frequently described as a state of "hyper-arousal." This heightened state of recursive anxiety not only increases the frequency of symptoms but also their intensity, as the limbic system becomes trapped in a persistent threat-detection mode. By leveraging targeted neuroplasticity, the NRI method aims to strengthen the brain's natural lateral inhibition. This process effectively "rewires" the pathway, decreasing the signal-to-noise ratio in the brain and allowing the nervous system to return to a state of homeostasis.
The efficacy of this approach is grounded in translational neuroscience and the study of re-entrant signaling. Peer-reviewed studies on non-invasive neuromodulation and habit reversal have shown that focused, high-state interventions can significantly reduce symptom severity by disrupting dysfunctional loops between the amygdala and the motor cortex. By participating in our research, patients contribute to a growing body of evidence that neurodivergent symptoms are not static; rather, they are dynamic processes that can be modulated through precise, evidence-based neuroplastic training.
We are currently enrolling patients for our clinical trial. If you or someone you know could benefit from our research, please contact us to learn more about eligibility and how to participate.
Sign up to join a clinical study designed to inhibit limbic loop frequency and intensity, providing relief from chronic anxiety and motor urgency through targeted neuroplasticity. This research focuses on disrupting dysfunctional limbic loops between the limbic system and the amygdala to break the cycle of recursive anxiety and motor urgency. The protocol is non-invasive, involves no pharmacological intervention, it is applied neuroscience, no hypnosis, no psycho therapy, and often makes a profound difference in one 30 minute session. More sessions are often unnecessary, but available according to your schedule.
This could be your breakthrough. Let's do this!
Brain Science
Fear makes every thing worse.
Disease is... Dis. Ease.
Chronic pain, suffering, anxiety, phobias and neuroses are evidence of a hardened limbic loop. Limbic loops are like brain muscles, they get stronger the more you stress them, but just like a muscle they can atrophy and weaken when you stop using them. The NeuroRecursion protocol empowers you to create a powerful, conscious "relief" from the old loop and create new neural pathways that liberate you from the chronic cycles of suffering your brain can be stuck in. By participating in our research, patients contribute to a growing body of evidence that neurodivergent symptoms are not static; they can be rewired and overcome through targeted neuroplasticity.
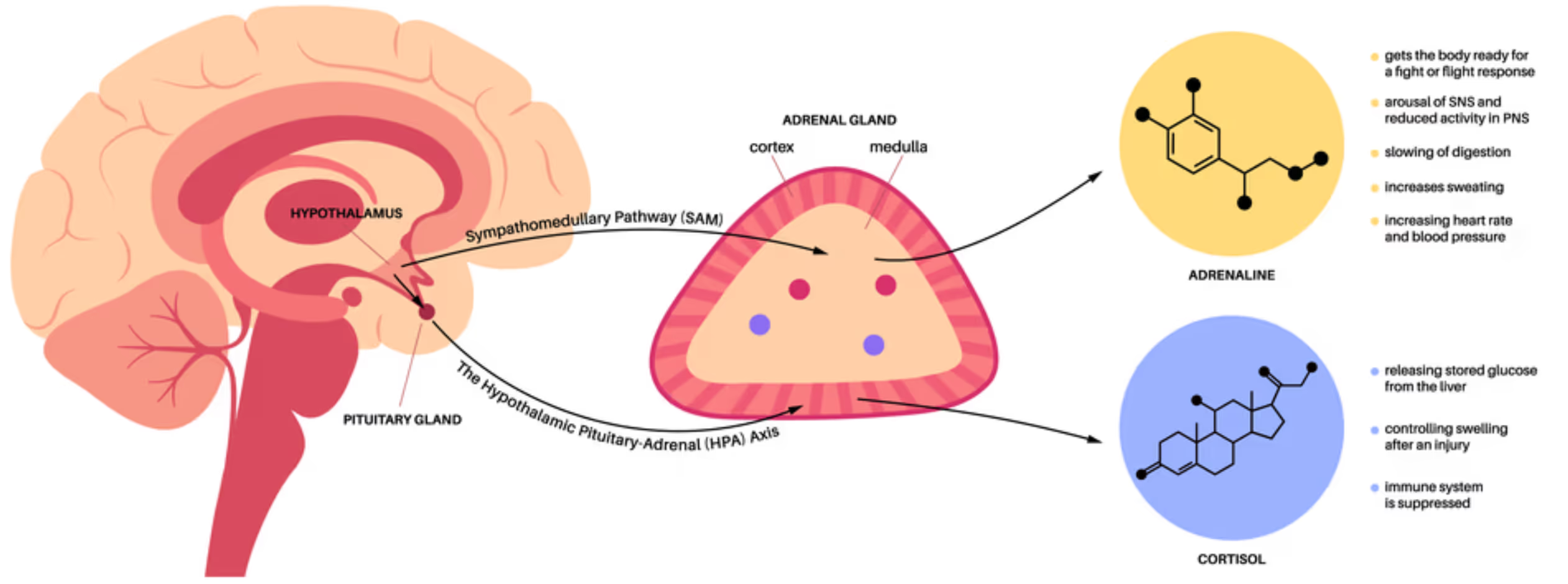
Because the limbic system cannot distinguish between a nightmare and reality, these loops trigger chronic physical stress. Persistent fear and anxiety cause the hypothalamus to over-stimulate the adrenal glands, flooding the body with cortisol and adrenaline. This chronic activation suppresses the immune system, increases systemic inflammation, and is a documented factor in the development of cardiovascular disease, gastrointestinal disorders, and metabolic syndrome. Fear also impairs neuroplasticity, making it difficult for the brain to rewire itself out of these loops. By targeting the limbic system and leveraging neuroplasticity, we can break these cycles and restore neurological health.
NeuroRecursion is a conversational protocol, similar to Exposure Therapy, but without the exposure, risk, or inconvenience, that leverages neuroplasticity to rewire these cycles. By leveraging the creative agency of the prefrontal cortex, we help you bypass old loops and create new neural pathways. While the brain possesses a natural elasticity, a biological tendency to snap back into established, familiar patterns, NeuroRecursion uses a deliberate "conscious trauma" breakthrough to shatter that resistance.
This process essentially highjacks the mechanics of the placebo effect. A placebo works because the brain's expectation of relief triggers a drop in the fear response, allowing the body to cease its defensive stress production and begin self-repair. NeuroRecursion creates a massive, conscious "relief" from the old loop during the breakthrough.
Our clinical trials focus on this high-impact, transformative event. To prevent the inevitable snap-back of neural elasticity, we also provide an ecosystem for ongoing maintenance that connects users with small group facilitators, 1 on 1 coaching, and seminars led by certified NeuroRecursion coaches to ensure the new neural landscape is reinforced and remains fixed in spite of neural elasticity.
Join us. The clinical trial is free, fast, and could be your breakthrough. Sometimes it's all you need.
References
Our work is grounded in the pioneering research and cognitive computational models developed by the world's leading neurological institutions.
- Harvard University - Department of Psychology; groundbreaking research on mental control, thought suppression, and the ironic processes underlying anxiety and intrusive thoughts Daniel Wegner
- MIT - Brain and Cognitive Sciences Division and McGovern Institute for Brain Research; pioneering work in neuroplasticity and neuromodulation Ann Graybiel
- Stanford University - Department of Neurobiology; leading research on neural circuits, habit formation, and therapeutic neurotechnology Carla Shatz
- University of Cambridge - Department of Psychology; advanced research in neurodevelopmental disorders and cognitive neuroscience Trevor Robbins
- University of California, Berkeley - Helen Wills Neuroscience Institute and Department of Neurobiology; world-class research in computational neuroscience, neuroplasticity, and circuit-level investigation of motor control and learning Gül Dölen
- University College London (UCL) - Institute of Neurology and Wellcome Centre for Neuroimaging; world-leading research in theoretical neuroscience and brain dynamics Karl Friston
- ETH Zurich (Switzerland) - Institute for Neuroinformatics and Brain Research Institute; world-leading research in computational neuroscience, neural circuits, and neuromorphic systems relevant to understanding recursive neural dynamics Giacomo Indiveri
- Max Planck Institute for Brain Research (Frankfurt, Germany) - Cutting-edge neurobiological research on brain connectivity and learning mechanisms Erin Schuman
- University of Melbourne (Australia) - Department of Anatomy and Neuroscience; pioneering research in brain plasticity, neuroinflammation, and neurorehabilitation Mary Galea
- McGill University (Canada) - Department of Psychology; pioneering research on memory reconsolidation and the neural basis of trauma and fear memory Karim Nader
- University of Tokyo - Institute of Medical Science; pioneering non-invasive neuromodulation and brain-computer interface research Yukiyasu Kamitani
- Tsinghua University (China) - School of Life Sciences and McGovern Institute for Brain Research; advanced research in neural circuits, brain imaging, and neuroplasticity Bo Li
- University of Geneva (Switzerland) - Swiss Centre for Affective Sciences; research on emotional memory, fear extinction, and reconsolidation-based therapy Olivier Hardt
- Indian Institute of Science (IISc) (Bangalore, India) - Centre for Neuroscience; leading research in computational neuroscience, neural plasticity, and brain circuit dynamics Aditya Murthy
- Icahn School of Medicine at Mount Sinai (New York, USA) - Departments of Psychiatry and Neuroscience; landmark research on memory reconsolidation and permanent fear neutralization Daniela Schiller
Sign Up
This could be your breakthrough. Let's do this!
Sign up to join a clinical study designed to inhibit frequency and intensity of neurological symptoms through targeted neuroplasticity. This research focuses on disrupting dysfunctional limbic loops between the limbic system and the amygdala to break the cycle of recursive anxiety and motor urgency. The protocol is non-invasive, involves no pharmacological intervention, it is applied neuroscience, no hypnosis, no psycho therapy, and often makes a profound difference in one 30 minute session. More sessions are often unnecessary, but available according to your schedule.
Results vary and are not guaranteed, but many patients experience significant relief after just one session. By participating in our research, you contribute to a growing body of evidence that neurodivergent symptoms are not static; rather, they are dynamic processes that can be modulated through precise, evidence-based neuroplastic training.
If you or someone you know could benefit from our research, please contact us to learn more about eligibility and how to participate.
Clinical Trials
Enrolling now!
Find your condition below and sign up to see if you qualify!
These conditions benefit from our technology that targets neuroplasticity and replaces hardened limbic loops with new neural pathways that increase your capacity for confidence, security, and joy.
We are continuously adding more. Don't see your condition? Sign up anyway. Also, the descriptions are brief summaries of complex conditions - your experience will differ and may be less severe than described. Also, you may have multiple conditions, so don't hesitate to sign up for more than one.
This could be your breakthrough. Let's do this! Don't hesitate.
Freedom, Power and Prosperity
Collaborative Innovation
This could be your breakthrough. Let's do this!
Imagine life without the fear that collaboration means losing credit, control, or safety, and the freedom to co-create boldly while preserving agency and authorship. Imagine shared work that multiplies intelligence instead of threatening identity. This is the breakthrough orientation of Collaborative Innovation.
The urge to collaborate springs from a deep recognition that some creations are only possible together. If you’ve ever felt the frustration of going it alone, or the thrill of shared discovery, you know the power of collaborative innovation. This desire is about dissolving the barriers of competition and fear, making space for a kind of creative synergy that feels effortless and alive. A key limiting belief is, "If I collaborate, I will be let down, controlled, or have my credit taken."
When you enter a state of collaborative flow, your nervous system synchronizes with those around you, quieting threat circuits and softening ego defenses. Conscious lucid engagement in the prefrontal cortex turns collaboration into a creative act of agency, where you can shape the exchange rather than brace against it. In that state, ideas amplify each other and failure loses its power to intimidate.
When collaborative innovation is chosen consciously, isolation and defensiveness stop running the show. This addresses the belief that collaboration inevitably costs safety or recognition, because the prefrontal cortex is actively proving that shared creation can preserve agency, authorship, and trust at once. Competition gives way to breakthrough, and what once seemed impossible alone becomes available in living cooperation.
This could be your breakthrough. Let's do this! Sign up now.
Visionary Courage
This could be your breakthrough. Let's do this!
Imagine life without the fear that bold action will end in catastrophic public failure, and the freedom to move decisively toward meaningful risk with strategic clarity. Imagine leading from conviction instead of bracing for collapse. This is the activating force of Visionary Courage.
Visionary courage is the rare ability to see possibility where others see only risk. If you’ve ever felt the pull to act boldly in the face of uncertainty, you know this desire intimately. It is not the absence of fear, but the willingness to move forward because meaning and purpose shine brighter than anxiety. Visionary courage is what fuels transformation, innovation, and the pursuit of dreams that matter. The limiting fear is, "If I take a big risk, I will fail publicly and ruin everything."
Your brain’s risk circuits are naturally tuned to avoid loss and pain, often holding you back from the unknown. Visionary courage changes this through conscious agency and lucid forecasting in the prefrontal cortex, which can reinterpret volatility as possibility rather than doom. In that state, the limbic system receives a new command: forward movement is not annihilation.
When courage is claimed consciously, paralysis and avoidance lose control. This rewrites the fear of catastrophic public failure, because the prefrontal cortex is actively teaching the nervous system that bold action does not equal identity collapse. Anxiety is converted into direction, setbacks into intelligence, and visionary courage becomes immediate permission to pursue what matters.
This could be your breakthrough. Let's do this! Sign up now.
Authentic Influence
This could be your breakthrough. Let's do this!
Imagine life without the fear that your voice will lose influence unless you perform for approval, and the freedom to lead through coherence, truth, and grounded authority. Imagine being respected because you are congruent, not because you are compliant. This is the power of Authentic Influence.
Authentic influence is the power that comes from living in alignment with your deepest values. When you act from a place of integrity, your presence naturally inspires trust and respect in others. This desire is about moving beyond the need for external validation, discovering the quiet strength that comes from self-regulation and congruence between your beliefs and actions. The limiting fear is, "If I stop performing for approval, I will lose influence and be ignored."
Your nervous system is exquisitely sensitive to authenticity, often recognizing it before your conscious mind does. Through lucid agency in the prefrontal cortex, integrity becomes a deliberate signal sent into the limbic system and into the social field around you. That coherence generates genuine connection, voluntary followership, and purpose without manipulation.
When authentic influence is enacted consciously, people-pleasing and self-doubt stop dictating your behavior. This resolves the fear of losing influence without performance, because the prefrontal cortex is actively demonstrating that credibility rises when you are coherent rather than compliant. Influence becomes an extension of truth, allowing you to lead and inspire without sacrificing integrity.
This could be your breakthrough. Let's do this! Sign up now.
Limbic Regulation Leadership
This could be your breakthrough. Let's do this!
Imagine life without the fear that stress and emotion will always overpower you, and the freedom to respond from calm command even under pressure. Imagine feeling your nervous system follow your conscious direction in real time. This is what Limbic Regulation Leadership makes possible.
Limbic regulation is the art of mastering your own nervous system, learning to generate a sense of calm and stability from within. If you’ve ever felt swept away by stress or anxiety, you know how powerful it can be to reclaim control over your internal state. This desire is about becoming the anchor in your own life, able to weather storms without being thrown off course. A central limiting fear is, "My emotions are uncontrollable, and stress will always overpower me."
Limbic regulation works by bringing conscious lucid command online in the prefrontal cortex, allowing you to recognize and interrupt overwhelm as it arises. Instead of waiting for the nervous system to calm itself slowly, agency steps in and redirects activation in real time. That gives you composure you can feel and project immediately.
When this capacity is engaged consciously, panic and reactivity lose their power. This directly addresses the fear of being permanently hijacked by stress, because the prefrontal cortex is proving to the limbic system that activation can be interrupted and reorganized now. Stability and self-trust become available as direct experience, giving you confidence and grace under pressure.
This could be your breakthrough. Let's do this! Sign up now.
Adaptive Resilience
This could be your breakthrough. Let's do this!
Imagine life without the fear that setbacks prove you are broken beyond repair, and the freedom to convert disruption into momentum, learning, and strength. Imagine challenge becoming raw material for evolution instead of a verdict against you. This is the immediate orientation of Adaptive Resilience.
Adaptive resilience is the ability to bend without breaking, to treat life’s volatility as a training ground for growth rather than a source of trauma. If you’ve ever faced setbacks or uncertainty, you know how vital it is to develop this trait. Adaptive resilience is about cultivating the flexibility to recover, learn, and thrive in the face of adversity. The core limiting belief is, "If I get knocked down, it proves I am broken and cannot recover."
Your brain is designed to metabolize stress as information, not just as a threat. Adaptive resilience leverages conscious agency and lucid reframing in the prefrontal cortex to reinterpret challenge as creative adaptation rather than damage. In that shift, fear and avoidance give way to curiosity and problem-solving.
When resilience is activated consciously, shutdown and despair lose their claim that you are broken. This directly challenges the belief of permanent brokenness, because the prefrontal cortex is showing the limbic system that recovery is available as an active choice rather than a distant hope. The unknown becomes navigable, and obstacles become material for personal evolution.
This could be your breakthrough. Let's do this! Sign up now.
High-Trust Bandwidth
This could be your breakthrough. Let's do this!
Imagine life without the fear that direct communication will be weaponized against you, and the freedom to speak with precision, openness, and protected trust. Imagine conversations that increase clarity and coordination instead of threat. This is the functional advantage of High-Trust Bandwidth.
High-trust bandwidth is the state where communication flows freely, unburdened by suspicion or hidden agendas. If you’ve ever struggled to be understood or felt the relief of total clarity, you know the value of this trait. High-trust bandwidth is about eliminating the friction of doubt, allowing you to connect, coordinate, and act with remarkable speed and precision. The limiting fear is, "If I communicate plainly, my words will be weaponized or used against me."
When transparency is chosen consciously, your nervous system stops wasting energy on threat detection or second-guessing. Lucid agency in the prefrontal cortex quiets the circuits that fuel anxiety and miscommunication, freeing bandwidth for creativity, collaboration, and precise response. This transforms both relationship and self-experience in the moment.
When high-trust communication is engaged consciously, suspicion and withdrawal stop setting the terms. This addresses the fear of being weaponized, because the prefrontal cortex can pair clear boundaries with clear speech and teach the limbic system that transparency can increase protection rather than reduce it. Trust becomes usable bandwidth for relationship and coordinated action.
This could be your breakthrough. Let's do this! Sign up now.
Intentional Culture Design
This could be your breakthrough. Let's do this!
Imagine life without the fear that systems are fixed and you cannot change your environment, and the freedom to architect conditions that support creativity, safety, and purpose. Imagine building contexts where your best self becomes easier to access. This is the agency inside Intentional Culture Design.
Intentional culture design is the conscious creation of rituals, habits, and environments that reinforce your deepest values and psychological health. If you’ve ever felt the difference between a nourishing environment and a toxic one, you know how powerful this process can be. Intentional culture design is about shaping the world around you to support your growth, creativity, and well-being. The limiting belief is, "My environment controls me, and I do not have enough power to change the system around me."
By engineering supportive structures, you teach your nervous system to expect safety, possibility, and connection. Intentional culture design is a creative act of agency in which the prefrontal cortex uses lucid imagination to reshape the environment so the limbic system receives new signals immediately. Threat and withdrawal give way to engagement and exploration because the field itself is being redesigned.
When culture design is enacted consciously, resignation and self-sabotage lose credibility. This directly counters helplessness, because the prefrontal cortex is proving that you can alter the system around you and thereby alter what the nervous system expects. Investment, creation, and belonging become active realities you can generate and extend to others.
This could be your breakthrough. Let's do this! Sign up now.
Strategic Patience
This could be your breakthrough. Let's do this!
Imagine life without the fear that if you do not act immediately you will lose everything, and the freedom to choose timing as power rather than panic. Imagine making moves from discernment, not urgency. This is the strategic advantage unlocked by Strategic Patience.
Strategic patience is the discipline to wait for the right moment, resisting the urge to react impulsively out of fear or anxiety. If you’ve ever regretted a hasty decision or wished for greater self-control, you know the value of this trait. Strategic patience is about cultivating the ability to pause, assess, and act with precision rather than compulsion. The limiting fear is, "If I do not act immediately, I will lose everything and miss my only chance."
Strategic patience works through conscious lucid command in the prefrontal cortex, which can override the limbic impulses that drive reactivity. Urgency and fear are reframed into discernment and timing because the mind is actively choosing the right moment rather than submitting to pressure. That makes precision possible without passivity.
When strategic patience is engaged consciously, impulsive action loses its hold. This directly addresses urgency panic by proving to your nervous system that pausing can improve outcomes rather than cause loss. Waiting becomes power, observation becomes leverage, and wise timing becomes a usable asset for navigating complexity with clarity.
This could be your breakthrough. Let's do this! Sign up now.
Courage, Love and Leadership
Radical Transparency
This could be your breakthrough. Let's do this!
Imagine life without the fear that being fully seen will get you rejected or punished, and the freedom to speak and live as your real self without self-censorship. Imagine showing up in relationships, work, and leadership from inner congruence instead of concealment. This is the immediate shift Radical Transparency invites: a life where truth and safety can coexist.
Radical transparency is a courageous act of self-liberation, inviting you to step out from behind the protective mask you’ve worn for years. When you allow your true thoughts and feelings to be seen, you begin to reclaim the energy once spent on hiding and self-censorship. This desire is not about reckless exposure, but about honoring your right to exist without the burden of secrecy, opening the door to genuine connection and self-acceptance. The limiting fear that often thwarts this virtue is, "If people see the real me, I will be rejected or punished."
On a neurobiological level, the habit of concealment keeps your limbic system in a constant state of alert, as if every truth is a potential threat. This process is not mechanical repetition but a creative act of agency, in which conscious, lucid activity in the prefrontal cortex confronts and rewrites the limbic prediction that honesty is dangerous. In that moment, new pathways open for self-compassion, coherence, and inner safety.
When openness is claimed consciously, the old limbic loop of fear and withdrawal is interrupted at the source. This directly disconfirms the belief that being seen guarantees rejection or punishment, because the prefrontal cortex is actively teaching the nervous system a new meaning for truth. Honesty stops feeling like exposure and starts feeling like relief, connection, and power. In this way, radical transparency moves you beyond survival mode into immediate freedom and belonging.
This could be your breakthrough. Let's do this! Sign up now.
Psychological Safety Anchoring
This could be your breakthrough. Let's do this!
Imagine life without the fear that one mistake will lead to humiliation or exile, and the freedom to take honest risks from an inner stance of safety and dignity. Imagine moving through challenge without bracing for social punishment. This is the living promise of Psychological Safety Anchoring.
The longing for psychological safety is deeply personal—a desire to finally relax into your own skin without the constant fear of judgment or reprisal. After years of bracing for criticism or exclusion, you may yearn for an internal sanctuary where you can take risks, express uncertainty, and share your true self without bracing for impact. Anchoring psychological safety is about building this inner refuge, a foundation for authentic growth and healing. A common limiting belief here is, "One mistake will get me humiliated, rejected, or exiled."
From a neurobiological perspective, psychological safety is not just a feeling but a measurable state of your nervous system. In this process, conscious agency and lucid imagination in the prefrontal cortex signal to the limbic system that safety can be generated, recognized, and chosen rather than passively awaited. That shift frees curiosity, expression, and connection immediately.
When safety is anchored consciously, the limbic patterns that kept you silent and guarded lose their authority. This directly weakens the belief that any mistake will end in humiliation or exile, because the prefrontal cortex is now defining error as survivable, repairable, and non-fatal to belonging. Anxiety gives way to openness and resilience, and psychological safety becomes a present operating state from which confidence and trust can move.
This could be your breakthrough. Let's do this! Sign up now.
Empathic Resonance
This could be your breakthrough. Let's do this!
Imagine life without the fear that emotional closeness will engulf you and erase your identity, and the freedom to connect deeply while staying fully anchored in yourself. Imagine intimacy that expands you instead of consuming you. This is the liberating state at the center of Empathic Resonance.
Empathic resonance is the longing to truly feel with others, to sense the subtle emotional currents that flow beneath words and actions. For many, this desire arises from a history of emotional disconnection or overwhelm, where attunement felt either impossible or unsafe. By nurturing empathic resonance, you reclaim the ability to connect deeply without losing yourself, discovering a new kind of emotional freedom. The limiting fear here is, "If I open to others, I will be engulfed and lose myself."
This capacity is rooted in the mirror neuron system and the limbic brain’s remarkable ability to synchronize with others. Here, conscious lucid awareness in the prefrontal cortex allows you to enter connection creatively rather than reactively, so empathy is guided by agency instead of overwhelm. That makes it possible to feel deeply while remaining anchored in your own center.
When empathic resonance is engaged consciously, the old limbic association between closeness and self-loss is disrupted. This directly addresses the fear of being engulfed, because the prefrontal cortex is showing the nervous system that intimacy and boundaries can coexist in the same moment. Connection stops requiring self-sacrifice and becomes mutual regulation, intimacy, and freedom from overwhelm.
This could be your breakthrough. Let's do this! Sign up now.
Inclusive Belonging
This could be your breakthrough. Let's do this!
Imagine life without the fear that your differences will get you excluded, and the freedom to belong without shrinking, performing, or hiding who you are. Imagine community as a place where authenticity increases safety instead of threatening it. This is the heart of Inclusive Belonging.
The longing to belong is one of the most fundamental human drives. If you’ve ever felt the sting of exclusion or the comfort of true acceptance, you know how powerful this desire can be. Inclusive belonging is about actively dissolving the old boundaries that separate you from others, allowing you to experience a sense of connection that is both safe and empowering. The limiting belief is, "If people see who I really am, I will be excluded for being different."
At the neural level, the brain’s social threat detectors are constantly scanning for signs of rejection or difference. Inclusive belonging changes that through conscious, lucid reframing in the prefrontal cortex, which teaches the limbic system to interpret difference as contribution rather than danger. That opens relationship, self-acceptance, and participation immediately.
When belonging is chosen consciously, withdrawal and defensiveness lose their mandate. This directly counters the expectation of exclusion, because the prefrontal cortex is showing the nervous system that authenticity and safety can coexist in the same social field. Inclusive belonging becomes a present foundation from which you can thrive in diversity and extend genuine welcome to others.
This could be your breakthrough. Let's do this! Sign up now.
Tribal Cohesion
This could be your breakthrough. Let's do this!
Imagine life without the fear that groups inevitably betray and closeness is unsafe, and the freedom to build intelligent trust in chosen community. Imagine belonging that is both warm and discerning. This is the social power of Tribal Cohesion.
The desire for tribal cohesion is rooted in the need for safety, belonging, and mutual support. If you’ve ever longed for a sense of unity or felt the pain of isolation, you understand the importance of this trait. Tribal cohesion is about building high-trust social loops that allow you to thrive, not just survive, in the company of others. The limiting fear is, "Groups always betray eventually, so closeness is dangerous."
At the neural level, rituals and feedback systems reinforce the bonds of loyalty and connection, creating a sense of shared purpose. Conscious lucid direction in the prefrontal cortex lets you enter these social fields creatively and selectively, so belonging is shaped by agency rather than blind fusion. The limbic system receives a new message: inclusion can be intelligent, chosen, and safe.
When tribal cohesion is formed consciously, suspicion and withdrawal lose their dominance. This softens the belief that all groups end in betrayal, because the prefrontal cortex is teaching the nervous system to distinguish true alliance from old threat templates. Belonging becomes strength, support, and coordinated flourishing inside a chosen community.
This could be your breakthrough. Let's do this! Sign up now.
Conflict Alchemy
This could be your breakthrough. Let's do this!
Imagine life without the fear that conflict inevitably destroys relationship, and the freedom to transform tension into repair, clarity, and stronger alignment. Imagine disagreement as an opening for deeper truth rather than a countdown to rupture. This is the alchemical edge of Conflict Resolution.
Conflict alchemy is the art of transforming friction into fuel for growth and understanding. If you’ve ever dreaded confrontation or longed for resolution, you know how challenging this process can be. Conflict alchemy is about learning to metabolize tension as creative energy, turning what once felt threatening into an opportunity for insight and connection. The limiting fear is, "Conflict always destroys relationships, so it is safer to avoid it or dominate it."
When you approach conflict with curiosity and openness, conscious lucid engagement in the prefrontal cortex overrides the old scripts of fight, flight, or freeze. Blame and defensiveness are replaced by empathy and problem-solving because the mind is actively reauthoring the meaning of tension. Conflict becomes creative energy rather than a threat signal.
When conflict alchemy is used consciously, avoidance and escalation lose their inevitability. This directly resolves the fear of relational destruction, because the prefrontal cortex is teaching the limbic system that rupture can become repair, deeper trust, and sharper agreement. What once felt like danger becomes a bridge to strength and understanding.
This could be your breakthrough. Let's do this! Sign up now.
Servant Leadership
This could be your breakthrough. Let's do this!
Imagine life without the fear that serving others will deplete, exploit, or erase you, and the freedom to lead through contribution with boundaries, reciprocity, and vitality. Imagine generosity that strengthens identity instead of draining it. This is the integrated power of Servant Leadership.
Servant leadership is the practice of leading from a place of abundance, security, and genuine care for others. If you’ve ever felt the fulfillment of helping someone grow or the satisfaction of contributing to a greater good, you understand the heart of this desire. Servant leadership is about focusing on the well-being of those around you, knowing that your own growth is intertwined with theirs. The limiting fear is, "If I serve others, I will be depleted, exploited, or rendered invisible."
When you embody servant leadership, your nervous system becomes a source of safety and empowerment. Conscious agency and lucid imagination in the prefrontal cortex recode service from scarcity into generativity, so the limbic system no longer reads contribution as self-erasure. Leadership becomes a creative force that catalyzes flourishing for everyone it touches.
When servant leadership is enacted consciously, self-protection and withdrawal lose their authority. This directly resolves the fear of depletion or exploitation by integrating service with boundaries, reciprocity, and sustainable contribution. Giving, receiving, and trust become part of the same empowered movement, allowing you to inspire, uplift, and create real impact.
This could be your breakthrough. Let's do this! Sign up now.
Anxiety, Panic & Social Threat
Generalized Anxiety Disorder
This could be your breakthrough. Let's do this!
Your nervous system learned to perpetually scan for danger and now produces anxious predictions and worry about everyday life situations. Threat-detection became chronic. Generalized Anxiety Disorder (GAD) is characterized by persistent, excessive worry about multiple everyday life domains (work, health, relationships, finances, future) that occurs more days than not for at least six months, causing significant distress and functional impairment. Individuals with GAD experience constant low-level anxiety background radiation, difficulty controlling worry, and often develop secondary physical symptoms (tension, fatigue, sleep disruption) from chronic activation.
The neurobiological mechanism involves amygdala hyperactivity and reduced prefrontal regulation where the threat-detection system remains persistently active without external threat trigger. The anterior cingulate cortex generates excessive error-detection and worry-rumination that keeps the anxiety system activated in a feedback loop. The insula becomes hyperactive in interoceptive threat-detection, meaning internal bodily sensations become misinterpreted as danger signals. The default mode network becomes overactive in catastrophic future-prediction and "what-if" scenarios. The nervous system learned that worry is protective (by predicting all possible dangers) and now uses worry as a false safety strategy that actually perpetuates anxiety.
Our technique recalibrates the threat-detection system and reduces amygdala hyperactivity through targeted limbic intervention. We dissolve the false belief that worry provides safety and restore accurate threat-assessment. Your nervous system ceases generating excessive worry and excess anxiety production. You experience stable baseline calm where worry no longer dominates consciousness and genuine safety is felt despite life's inherent uncertainties.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Social Media Anxiety Disorder
This could be your breakthrough. Let's do this!
Your nervous system treats social media platforms as high-stakes social evaluation environments where judgment is constant. It's time to recalibrate social threat perception. Social media anxiety disorder is a specific manifestation of anxiety related to social media use, characterized by fear of missing out (FOMO), anxiety about negative social judgment on platforms, compulsive social comparison, and anxiety-driven social media checking and posting behaviors. Individuals with social media anxiety experience intense anxiety if separated from social media, catastrophic interpretations of lack of engagement or 'likes,' and a pervasive sense that their social media presence determines social acceptability and status. This anxiety is amplified by algorithm-driven content and psychological manipulation in social media platform design.
The neurobiological mechanism involves amygdala hyperactivity in response to social evaluation threat combined with dopamine-driven behavioral addiction. Social media platforms are specifically engineered to trigger dopamine-reward cycles (likes, comments, shares) that create compulsive checking behaviors. Simultaneously, the algorithmic curation shows content that triggers social comparison on the insula and amygdala threat-activation in response to perceived social exclusion (FOMO). The amygdala becomes conditioned to interpret lack of engagement as social rejection. Anxiety about posts or lack of engagement drives checking and posting cycles. The prefrontal cortex loses regulatory capacity as the amygdala and striatum (reward system) hijack decision-making.
Our technique dissolves the social-evaluation threat perception specific to social media through targeted limbic recalibration. We interrupt the dopamine-driven compulsive checking and restore genuine social evaluation capacity grounded in real relationships rather than platform-based metrics. Your nervous system regains capacity to engage with social media without anxiety-driven compulsion or social comparison rumination. This isn't digital detox or social media limiting. It's recoding of how your nervous system processes social threat and reward in digital contexts. You experience freedom from platform-driven anxiety and restored capacity for genuine social connection.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Health Anxiety and Hypochondriasis
This could be your breakthrough. Let's do this!
Your nervous system misinterprets neutral bodily signals as life-threatening disease. It's time to recalibrate the sensitivity. Health anxiety is characterized by preoccupation with having or acquiring serious illness despite medical reassurance, hypervigilance to bodily sensations, excessive health-seeking behaviors or avoidance of medical care, and significant distress and functional impairment. Individuals with health anxiety experience persistent catastrophic interpretations of normal bodily functions (heartbeats, aches, digestive sounds) as evidence of serious pathology. This creates anxiety-driven symptom escalation where worry about symptoms amplifies physical sensations, which amplifies worry—a vicious self-perpetuating cycle. Health anxiety costs billions in unnecessary medical care and creates immense suffering despite repeated normal test results.
The neurobiological mechanism involves amygdala hyperactivity in response to interoceptive (bodily) signals combined with a failure of the brain's threat-extinction system to learn from repeated negative test results. The insula—which processes internal bodily signals—becomes hypersensitive, amplifying awareness of normal physiological variations. When bodily signals enter consciousness, the amygdala rapidly interprets them as threat before conscious assessment occurs. The brain's threat-extinction system fails to update despite evidence of safety (normal medical tests), suggesting a specific malfunction in how the amygdala processes health-related reassurance.
Our technique recalibrates the amygdala's interpretation of bodily signals and restores the threat-extinction system through targeted limbic intervention. We reduce insula hypersensitivity and restore accurate threat-assessment in response to bodily sensations. Intrusive catastrophic health thoughts recede as the nervous system regains confidence in distinguishing serious disease from normal body function. This isn't reassurance-seeking or meditation. It's recoding of how your nervous system interprets interoceptive signals. You experience freedom from health preoccupation and restored trust in your body's signals.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Agoraphobia/Social Phobia - Fear of Open/Crowded Spaces
This could be your breakthrough. Let's do this!
Your nervous system has decided the world is a trap. It's time to set it free. Agoraphobia is a panic/anxiety disorder characterized by intense fear and avoidance of situations from which escape might be difficult or embarrassing, particularly open spaces, crowds, public transportation, or being away from home. Severe agoraphobia can become completely disabling, with individuals becoming housebound and dependent on others for basic functioning. Social phobia often accompanies or overlaps with agoraphobia, with fear of negative social evaluation compounding the fear of being trapped in public spaces.
The neurobiological mechanism involves a heightened threat response to situations where the individual perceives limited escape options or potential judgment from others. The amygdala becomes sensitized to crowd-related cues, open spaces, and social presence, triggering panic attacks that feel bodily overwhelming and create catastrophic thoughts about losing control or having a medical emergency. The individual then begins avoiding situations that triggered panic, which reinforces the amygdala's belief that these situations are dangerous.
Our technique dismantles the agoraphobia trap through targeted recalibration of the escape-threat loop and social evaluation neural networks. We identify the specific beliefs and amygdala hijacks that created the prison, then restore genuine freedom and agency through creative reprogramming. Fear of crowds and open spaces transforms into confidence and mobility. This isn't exposure therapy or gradual reentry. It's swift recoding of the threat signature. You reclaim previously-avoided spaces, public transportation, and independence at striking speed.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Panic Disorder & Agoraphobia - Catastrophic Fear Response
This could be your breakthrough. Let's do this!
Your nervous system learned that normal sensations are harbingers of catastrophe and that certain places are traps where catastrophe will unfold inescapably. Panic disorder is characterized by unexpected, recurrent panic attacks (sudden, intense periods of fear or discomfort with physical symptoms like chest pain, shortness of breath, dizziness, or fear of dying) followed by persistent worry about having more attacks, and often agoraphobia (avoidance of situations or places where escape might be difficult or help unavailable if panic occurs). The person's world progressively shrinks as they avoid situations that have triggered panic or could trigger it. What began as unexpected panic attacks becomes a prison where the person can no longer drive, use public transit, be in crowds, or venture far from home.
The neurobiological mechanism involves a catastrophic misfiring of the interoceptive threat-detection system combined with amygdala hyperactivity and inaccurate body-signal interpretation. The insula (which monitors internal body signals) becomes hyperactive and begins generating disaster-predictions from normal sensations: "This rapid heartbeat means I'm having a heart attack," "This breathlessness means I'm suffocating," "This dizziness means I'm losing control." The amygdala becomes hyperresponsive to these misinterpreted signals, generating acute threat-response (fight-or-flight sympathetic activation) to what are actually harmless sensations. This triggers a vicious cycle: normal autonomic activation is misinterpreted as danger, generating anxiety, which generates more autonomic activation, which is misinterpreted as worsening catastrophe. The anterior cingulate cortex becomes locked in catastrophic prediction loops. The dorsolateral prefrontal cortex loses capacity to reality-test the catastrophic interpretations ("That's not a heart attack, it's anxiety"). Escape from the situation temporarily relieves anxiety, creating a powerful learned association: "I was dying but I escaped and survived." This makes avoidance intensely rewarded. Over time, agoraphobia develops as the person restricts their world to avoid triggering situations.
Our technique recalibrates the insula's body-signal interpretation and transforms its disaster-prediction mode through targeted limbic intervention. We rebuild accurate threat/non-threat assessment of internal sensations. We help the amygdala recognize that the panic response itself, while intensely uncomfortable, is not dangerous. We recalibrate the anterior cingulate's catastrophic prediction circuits. We systematically reduce the learned association between escape and safety by supporting the person through discomfort without escape. The dorsolateral prefrontal cortex regains capacity for rational evaluation during panic. You experience decreased panic attack frequency and intensity, tolerance for the physical sensations of anxiety without interpreting them as catastrophe, expanded world as agoraphobic avoidance resolves, and the freedom to move through the world without terror-driven restriction.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Hyperhidrosis - Emotional Sweating, Social Fear & Sympathetic Overdrive
This could be your breakthrough. Let's do this!
Your sympathetic nervous system may be treating ordinary social exposure like an emergency. Hyperhidrosis involves excessive sweating beyond what temperature or exertion alone would explain, commonly affecting the palms, feet, underarms, or face. For many individuals, the most disabling part is not the sweat itself but the dread of being seen sweating, shaking hands, staining clothing, or being judged as anxious, unclean, or weak.
The neurobiological mechanism involves overactivation of sympathetic output to sweat glands combined with social-threat conditioning. The amygdala interprets observation, performance, or interpersonal contact as danger, causing immediate autonomic escalation. Once sweating begins, the insula and self-monitoring systems lock onto it as proof of social threat, which amplifies the body's output further. The result is a rapid loop: fear of sweating creates more sweating, and the visible symptom becomes a chronic trigger for shame and avoidance.
Our technique targets the social-threat coding and autonomic overreaction that keep emotional sweating self-reinforcing. This is not a replacement for dermatologic, neurologic, or surgical care such as antiperspirants, Botox, medication, or sympathectomy when those are indicated. It addresses the fear-sweat loop that makes the condition far more functionally impairing. You experience reduced anticipatory dread, less escalation in watched or evaluated situations, and a nervous system that no longer treats social exposure as a signal to flood the body with sweat.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Pain & Suffering - Context-Driven Pain Amplification
This could be your breakthrough. Let's do this!
Some people love pain. If you're one of them, you don't need this, but if you're like most of us, you suffer about pain, and that suffering is often more debilitating than the pain itself. This can help.
Your pain is real, but the suffering built around pain is being actively amplified by the brain. Pain is not a passive meter reading from injured tissue. It is a context-sensitive protection output that the nervous system increases, decreases, suppresses, or prioritizes depending on what it thinks matters most. You already know this neurologically: people can ignore major pain when trauma is severe enough, when adrenaline is high enough, or when the task is critical enough. The brain can suppress pain during combat, crisis, rescue, performance, or shock. In short, your brain controls your experience of pain. This process is for people whose pain has become entangled with fear, anticipation, monitoring, helplessness, and suffering about the pain itself. This isn't about will power, it's about brain power, and this process will help you harness and use the pain signal rather than suffer about it. In short, pain will motivate you instead of stop you.
The neurobiological mechanism involves descending pain modulation, salience assignment, and threat interpretation. The periaqueductal gray, anterior cingulate cortex, insula, amygdala, prefrontal cortex, and spinal gating networks continuously determine whether nociceptive input should be dampened, ignored, highlighted, or escalated. When the brain concludes that immediate survival or action takes priority, endogenous opioids, noradrenergic activation, attentional narrowing, and top-down suppression can markedly reduce pain perception. When the brain instead codes the pain as ominous, uncontrollable, identity-relevant, or predictive of further harm, those same systems shift toward amplification. Catastrophizing, hypervigilance, and pain-focused prediction increase salience and suffering, often making the pain broader, louder, and more consuming than the underlying signal alone.
Our process targets the pain-suffering limbic loop directly. It won't necessarily reduce the pain, but it will reduce the suffering. This is not denial, distraction, or generic pain management. It is targeted recalibration of the neural systems that decides how much suffering gets layered onto sensation. As that threat architecture collapses, pain often becomes less dominant, less frightening, more precise, and substantially easier to live with. You may even find that the pain becomes a resource for motivation, action, and connection rather than a source of suffering. This is not about changing the pain signal itself, but about changing how your brain processes and responds to it. When the suffering loop is broken, you can experience relief even if the pain remains.
At this point, wouldn't you love to be one of those people who enjoy it? Might as well go for it.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Specific Phobias & Existential Fear
General Fears & Phobias
This could be your breakthrough. Let's do this!
Specific objects or situations trigger your amygdala as if they were survival dangers. Your threat-detection system learned a false positives. Phobias are intense, irrational fears of specific objects or situations that pose little actual danger but trigger severe anxiety and avoidance behaviors. Whether it's clouds, holes, snow, tears, bananas, or countless other specific stimuli, phobias cause individuals to arrange their lives around avoidance and experience significant functional impairment despite intellectually knowing the fear is irrational.
The neurobiological mechanism involves classical conditioning where a neutral stimulus became associated with threat through single-exposure or vicarious learning. The amygdala now automatically detects that specific stimulus and triggers a threat response before conscious awareness engages. The stimulus-threat association becomes so entrenched that despite cortical knowledge that the object is safe, the amygdala continues firing, generating the characteristic experience of irrational but overwhelming fear. Avoidance negatively reinforces the fear by preventing amygdala extinction through habituation.
Our technique dissolves the specific stimulus-threat association through targeted amygdala recalibration. We break the conditioned fear response and restore accurate threat assessment of the specific stimulus. Your nervous system ceases to respond with fear when encountering the phobic object. You experience rapid freedom from the specific phobia and restored capacity to engage with previously avoided situations.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Cynophobia - Fear of Dogs
This could be your breakthrough. Let's do this!
Your amygdala filed a threat report on dogs years ago. It's time to consciously revise that file. Cynophobia, the fear of dogs, is a specific phobia affecting individuals who have experienced prior negative dog-related experiences or have learned fear responses through observation or instruction. Individuals with cynophobia experience intense anxiety in the presence of dogs or even at the sound of barking, and often engage in significant avoidance of parks, neighborhoods, and social situations where dogs might be present. This phobia can severely restrict social participation and outdoor activities, particularly in communities where dogs are common pets.
The neurobiological mechanism often involves conditioning where a negative dog-related experience (being bitten, chased, or jumped on) becomes associated with threat in the amygdala. The dog's sudden movements, loud bark, or physical proximity can trigger an automatic threat response that the individual experiences as overwhelming fear. Unlike evolutionary fears like arachnophobia, cynophobia is typically learned, but once conditioned, the amygdala's threat response becomes equally automatic and difficult to override.
Our technique dissolves the learned dog-threat association through targeted limbic recalibration. We interrupt the automatic fear cascade and replace it with genuine curiosity and trust. The amygdala's threat classification of dogs transforms fundamentally. This isn't gradual systematic desensitization or forced exposure. It's swift reprogramming at the neurological level. You move from panic at the sound of barking to authentic pleasure in the company of dogs, accessing parks and social situations that seemed impossible before.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Astraphobia - Fear of Storms/Thunder/Lightning
This could be your breakthrough. Let's do this!
Your amygdala treats storms as threats the way it was programmed to. Conscious recalibration rewrites that program. Astraphobia, the fear of storms, thunder, and lightning, is a specific phobia characterized by intense anxiety and panic during thunderstorms or when storms are forecast. Individuals with astraphobia often experience hypervigilance to weather forecasts, avoidance of outdoor activities during stormy seasons, and significant distress when storms occur. This phobia can restrict travel, limit outdoor recreation, and create significant anxiety during otherwise normal weather patterns, particularly for those living in regions with frequent thunderstorms.
The neurobiological mechanism involves both realistic threat perception and amygdala hyperreactivity to sudden, loud noises and visual stimuli. Thunder and lightning are inherently startling to the human nervous system due to their unpredictable, loud, and intense nature, but individuals with astraphobia show exaggerated amygdala responses that trigger panic far beyond the actual risk level. The unpredictability of storms compounds the threat response, as the individual cannot anticipate when the next sound or flash will occur, creating sustained anxiety throughout the storm.
Our technique recalibrates the storm threat association through targeted creative reprogramming. We dissolve the exaggerated amygdala response to thunder and lightning and replace it with resources, awe, and calm presence. Unpredictability that once triggered sustained panic becomes manageable. This isn't gradual habituation or forced exposure. It's swift recoding of threat classification. Your relationship with storms transforms fundamentally. Travel and outdoor recreation during storm seasons becomes accessible with newfound freedom.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Arachnophobia - Fear of Spiders
This could be your breakthrough. Let's do this!
Your amygdala has misclassified spiders as predators. Let's correct the file. Arachnophobia is one of the most common specific phobias affecting a significant portion of the population. Despite the fact that most spiders are harmless to humans, individuals with arachnophobia experience intense panic, avoidance, and significant distress when encountering a spider or even a picture of one. This phobia can severely limit activities outdoors, in basements, or in other spaces where spiders may be present.
The neurobiological mechanism of arachnophobia involves an evolutionary predisposition where the amygdala has been primed to detect certain threats with heightened sensitivity. A single negative experience or even witnessing another person's fear response can condition the amygdala to perceive spiders as life-threatening, creating a rapid, automatic fear response that bypasses higher-order cognition. The sight of a spider triggers immediate amygdala activation before conscious awareness is fully engaged, leading to panic and avoidance.
Our technique recodes the amygdala's threat classification through targeted creative intervention. We identify the specific fear beliefs and limiting assumptions about spiders, then use precise limbic recalibration to replace the threat file with a new classification: benign or even fascinating. This isn't desensitization, exposure therapy, or gradual accommodation. It's recoding of the threat signature at its source. Your nervous system shifts from panic-on-sight to curiosity-on-sight within the first session. Individuals access activities like hiking, gardening, and relaxation in previously-feared spaces. When your amygdala reclassifies correctly, your freedom expands.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Ophidiophobia - Fear of Snakes
This could be your breakthrough. Let's do this!
Your evolutionary threat detection system has been running on a hair trigger. It's time to attenuate the alarm. Ophidiophobia is a deeply rooted primal fear affecting many individuals, often triggered by an inborn predisposition combined with learned responses. Those affected experience panic, hypervigilance, and avoidance behaviors that can severely limit activities like hiking, camping, travel to certain regions, or even simple yard maintenance. The fear often persists despite intellectually knowing most snakes are harmless.
The neurobiological basis of ophidiophobia exists at the intersection of evolutionary preparedness and conditioned learning. The amygdala contains rapid detection pathways optimized for predation threats including snakes, meaning humans are inherently biased to learn fear responses quickly when exposed to snakes. This evolutionary advantage becomes a liability when the amygdala's threat threshold becomes hypersensitized through trauma, vicarious learning, or even cultural messaging, creating a fast-acting automatic fear response that dominates conscious experience.
Our technique targets the amygdala's threat detection architecture, recalibrating the sensitivity and classification of snake-related stimuli. We dissolve the amygdala hijack through precise limbic reprogramming, where the automatic fear cascade is interrupted and replaced with resources, curiosity, and calm. This isn't gradual exposure or cognitive reframing. It's swift recoding of the threat signature at the neurological level. Your nervous system learns to perceive snakes as non-threatening entities within a single session, often with lasting transformation. When your amygdala recalibrates, your freedom to explore expands substantially.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Claustrophobia - Fear of Enclosed Spaces
This could be your breakthrough. Let's do this!
Your nervous system learned that confined spaces meant danger. Lucid transformation teaches it the difference between then and now. Claustrophobia, the fear of enclosed spaces, is a specific phobia characterized by intense anxiety when in small, confined spaces such as elevators, small bathrooms, closets, or confined areas without clear exits. Individuals with claustrophobia often experience panic attacks in these situations and engage in significant avoidance that can substantially restrict their daily functioning, limiting their ability to use elevators, fly, or work in certain environments. The fear often involves catastrophic thoughts about being trapped, unable to escape, or suffocating.
The neurobiological mechanism combines threat responses to spatial confinement with a heightened sensitivity to perceived loss of control and escape routes. The amygdala perceives enclosed spaces as threatening, triggering both anxious anticipation before entering and panic if actually confined. Hypervigilance to bodily sensations (breathing, chest tightness, temperature) combines with catastrophic thinking to create escalating anxiety. The sensation of walls closing in activates interoceptive threat detection alongside spatial threat detection.
Our technique recalibrates the confinement-threat association and interoceptive alarm through targeted creative intervention. We dissolve both the spatial threat perception and the body-focused anxiety hijack. Your nervous system learns that enclosed spaces are manageable. This isn't gradual progressive exposure forcing through discomfort. It's swift recoding of threat classification. You access elevators, aircraft, confined spaces, and new possibilities with composed confidence.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Trypanophobia - Fear of Needles/Injections
This could be your breakthrough. Let's do this!
Your nervous system conflates a tiny puncture with mortal danger. That's affecting your health. Trypanophobia, the fear of needles or injections, is a specific phobia that can have serious health consequences as it often leads individuals to avoid necessary medical procedures, vaccinations, and dental care. Individuals with trypanophobia experience intense anxiety, panic, fainting, or avoidance when facing needle-related medical interventions. This phobia not only impacts individual health outcomes but can also have public health implications when it prevents people from receiving vaccinations or routine preventive care.
The neurobiological mechanism involves a heightened threat response to potential pain combined with a unique vasovagal response where seeing or anticipating needles triggers parasympathetic activation that causes fainting. Many individuals report that their fear intensifies when they observe the injection itself, creating a temporary loss of consciousness that paradoxically reinforces their fear of needles. The blood-injection-injury phobia category (of which trypanophobia is a part) uniquely involves this fainting response due to the specific way the amygdala of susceptible individuals processes injury threat.
Our technique recalibrates the needle-threat association through targeted creative intervention. We dissolve the amygdala hijack and the vasovagal fainting mechanism simultaneously, replacing them with genuine resources and calm presence. Threat coding around needles transforms at the neurological level. This isn't gradual exposure or continued avoidance. It's swift recoding of injury threat perception. You access necessary medical procedures, vaccinations, and dental care with composed capability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Acrophobia - Fear of Heights
This could be your breakthrough. Let's do this!
Your inner ear is screaming safety warnings your conscious mind finds ridiculous. Let's recalibrate that amplifier. Acrophobia, the fear of heights, is a specific phobia involving intense fear and panic when at elevation or looking down from a height. Unlike most other phobias, acrophobia has a strong physiological component as our vestibular system (which controls balance) naturally creates unease at heights as a survival mechanism. However, in individuals with acrophobia, this natural caution escalates into overwhelming panic, avoidance of bridges, tall buildings, and mountains, significantly restricting their activities and travel.
The neurobiological mechanism combines vestibular dysregulation with amygdala hyperreactivity. The vestibular system sends signals of imbalance and threat to the amygdala, which becomes hyper-responsive and triggers a panic response. Individuals often catastrophize about falling, losing control, or having a panic attack at height, creating a feedback loop where anxiety about the anxiety further amplifies the threat response. The brain enters a state of hypervigilance to falling-related cues.
Our technique engages the intersection of vestibular and limbic signal processing through targeted creative reprogramming. We stabilize vestibular function while simultaneously recalibrating the amygdala's threat assessment for heights. The automatic fear cascade transforms into genuine confidence and presence. This isn't gradual exposure or forced habituation. It's swift recoding of the threat signature and vestibular integration. Individuals access bridges, buildings, and mountains with the courage that heights can inspire, not the panic they once triggered.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Thanatophobia - Death Anxiety
This could be your breakthrough. Let's do this!
Death feels imminent and unpredictable. Your nervous system learned that death is a present danger rather than a distant eventual reality. Thanatophobia is an abnormal fear of death or dying, characterized by persistent, intrusive thoughts about one's death or others' deaths, intense anxiety when death is contemplated, and often panic attacks triggered by mortality reminders. Individuals with thanatophobia may engage in excessive health-checking, avoidance of situations associated with death, or complete preoccupation with staying alive, leading to severe functional impairment.
The neurobiological mechanism involves an amygdala that has been conditioned to perceive death awareness as immediate and personal threat. The orbitofrontal cortex fails to accurately assess actual death probability—treating death as equally likely whether one is healthy or ill, young or old. Mortality reminders (sirens, aging parents, news reports) trigger an amygdala hijack that floods the system with panic neurochemicals. The anterior cingulate cortex generates obsessive death rumination that reinforces amygdala sensitivity. Ironically, the hypervigilance to death becomes an obsessive mental habit that consumes quality of life in the present.
Our technique recalibrates death perception and dissolves the morbid obsession pattern through targeted limbic intervention. We restore accurate probability assessment and emotional proportionality around mortality. Your nervous system ceases to treat death awareness as immediate threat. You experience acceptance of mortality, freedom from intrusive death thoughts, and restored capacity to engage fully in life.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Aerophobia - Fear of Flying
This could be your breakthrough. Let's do this!
Your nervous system believes the cabin is a metal tube hurtling toward disaster. Except you're not. Aerophobia, the fear of flying, affects a substantial portion of the population and can range from mild anxiety to complete avoidance of air travel. Individuals with aerophobia experience intense anxiety before and during flights, often experiencing panic attacks, catastrophic thoughts about crashes, and significant avoidance that impacts travel, career opportunities, and vacation plans. For many, aerophobia severely restricts their life choices and leads to feelings of shame and limitation.
The neurobiological mechanism combines actual lack of control (the flight is controlled by the pilot) with vestibular dysregulation (the unusual sensations of flight confuse the balance system) and catastrophic thinking patterns. The amygdala perceives the combination of altitude, enclosed space, and loss of control as existential threat, triggering panic responses that feel overwhelming and uncontrollable. Hypervigilance to flight-related bodily sensations (turbulence, slight noises, pressure changes) further amplifies anxiety.
Our technique targets the convergence of fears through precise limbic reprogramming. We dissolve the catastrophic beliefs and amygdala threat associations one by one, replacing them with genuine confidence in safety and capability. Automatic panic to flying stimuli transforms into calm presence. This isn't graduated exposure or white-knuckle coping. It's swift recoding of all the threat signals that converge in air travel. You access safe, relaxed international travel at striking speed.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Chronophobia - Fear of Time/Future
This could be your breakthrough. Let's do this!
Time feels like a threat. Your nervous system learned that the future is dangerous and mortality is imminent. Chronophobia is characterized by an irrational fear of time passing, the aging process, death, or the future. Individuals with chronophobia experience intense anxiety when thinking about aging, time's passage, or inevitable death, leading to obsessive time-checking, difficulty functioning in the present, and pervasive dread about mortality. This often co-occurs with health anxiety and perfectionism, as individuals try to "race against time" to accomplish everything before death.
The neurobiological mechanism involves an overactive amygdala that perceives time's passage and mortality awareness as existential threat. The insular cortex becomes hyperactive in processing bodily sensations related to aging and the passage of time. When the amygdala detects thoughts about time, aging, or death, it triggers a threat response that becomes associated with temporal awareness itself. The anterior cingulate cortex generates persistent rumination about mortality, and the prefrontal cortex fails to regulate this catastrophic thinking. Paradoxically, hypervigilance to time's passage actually intensifies the subjective experience of time urgency and threatens peace with the present moment.
Our technique recalibrates the amygdala's threat perception around time and mortality through targeted limbic intervention. We dissolve the existential threat association with temporal awareness and restore presence and acceptance of mortality. Your nervous system ceases to treat time's passage as danger. You experience peace in the present moment, healthy perspective on aging, and freedom from mortality obsession.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Achievemeophobia - Fear of Success, Power, and the Jonah Complex
This could be your breakthrough. Let's do this!
Your nervous system may be interpreting the prospect of high achievement as a threat to your social safety and identity. Achievemeophobia and the Jonah Complex involve an unconscious avoidance of your own potential; often driven by the dread of isolation, the burden of new responsibilities, or the fear that power will lead to moral corruption. For many, the most paralyzing aspect is the belief that success will alienate friends or make one a target for resentment and judgment.
The neurobiological mechanism involves a conflict between the drive for self actualization and the evolutionary need for tribal belonging. When you approach a threshold of significant power or wealth, the amygdala signals a social survival threat; fearing that rising above the group will result in ostracization. This creates a self sabotaging loop where the brain treats professional or personal breakthroughs as signals to retreat into mediocrity. The result is a chronic pattern of hesitation and the active avoidance of the very destiny you desire.
Our technique starts with your beliefs about "powerful people", authority, and extreme wealth. We identify your social currency and what threatens it. These beliefs are likely limiting beliefs about what you deserve, who you are allowed to be, and how others will perceive you. Together, we target the threat encoding associated with expansion and high status. We work to decouple the concept of power from the fear of corruption and social loss. You will be newly inspired to be the best Gazillionaire on the planet! This process addresses the autonomic brakes that stop you from finishing projects or accepting leadership roles. You experience a recalibrated nervous system that views success as a safe, if not critically important, and sustainable state rather than a dangerous departure from your identity and community.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Chrometophobia - Extreme Fear of Money & Financial Anxiety
This could be your breakthrough. Let's do this!
Your nervous system perceives money itself as a threat—handling cash, making financial decisions, or even thinking about finances triggers acute anxiety and avoidance. Chrometophobia is an extreme, irrational fear of money characterized by intense anxiety about mismanaging funds, the physical handling of cash, paying bills, or any financial transaction. Unlike healthy financial caution, chrometophobia involves a phobic response where the person's amygdala has encoded money-related activity as existentially threatening. The individual may avoid handling currency entirely, refuse to pay bills, experience panic attacks when confronted with financial decisions, or create elaborate avoidance systems that paradoxically create worse financial consequences. Common presentations include inability to access bank accounts, unopened bills, avoidance of shopping, or complete financial helplessness despite having the capability to manage finances.
The neurobiological mechanism involves hyperactivation of the amygdala in response to financial stimuli, combined with dysregulation of the anterior insula (which generates feelings of wrongness or threat). Often, the person has encoded money with early trauma: family violence centered around money, severe poverty with associated deprivation or shame, financial abandonment or betrayal, or messages that "money is evil" or "you don't deserve it." The ventromedial prefrontal cortex fails to generate accurate threat-assessment of money versus actual existential threats, and instead encodes financial engagement as equivalent to mortal danger. The anterior cingulate cortex becomes hyperactive in conflict-monitoring when financial decisions must be made. The dorsolateral prefrontal cortex's rational planning capacity becomes suppressed by amygdala-driven threat-response. The insula generates persistent bodily distress in the presence of money or financial stimuli.
Our technique dissolves the amygdala's false threat-encoding of financial activity by directly recalibrating the neural circuits that have encoded money as dangerous. We reprogram the anterior insula so financial stimuli (cash, bills, bank statements) register as neutral or manageable rather than generating internal wrongness-signals. We restore the ventromedial prefrontal cortex's capacity for accurate threat-assessment so rational financial evaluation becomes possible. We address any underlying trauma that created the money-threat association and reprogram those neural pathways. We restore the dorsolateral prefrontal cortex's capacity to engage in rational financial planning. You experience rapid elimination of acute anxiety in financial situations, ability to handle money and make financial decisions without panic, restored access to banking and financial management, and the capacity to engage with finances as normal adult functioning rather than as survival threat.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Mood, Identity & Body Image
General Mood Disorders
This could be your breakthrough. Let's do this!
Your mood system became dysregulated and now generates states that interfere with your life. Whether cyclical, reactive, mixed, or persistent, nervous system dysregulation created a mood problem. Mood disorders encompass diverse conditions affecting emotional regulation, including dysthymia (persistent low mood), cyclothymia (cycling mood states), mixed mood states, and other patterns that significantly impair functioning and wellbeing. Individuals experience either persistently depressed mood or mood cycling that disrupts relationships, work, sleep, and overall quality of life.
The neurobiological mechanisms vary across mood disorder types but generally involve dysregulation of monoamine systems (serotonin, dopamine, norepinephrine), hyperactivity or hypoactivity in the amygdala and prefrontal cortex, disruption of circadian rhythm regulation, and abnormalities in HPA axis stress response. Chronic stress, trauma, substance use, sleep disruption, or other factors dysregulate these systems and create persistent mood dysfunction. The nervous system becomes stuck in patterns of mood generation that persist regardless of external circumstances.
Our technique identifies the specific dysregulation pattern and restores balanced mood regulation through targeted limbic intervention. We dissolve the driving mechanisms behind disordered mood states and restore healthy mood cycling or sustained stable affect. Your nervous system regains capacity for emotional resilience and appropriate mood response to circumstances. You experience freedom from mood disorder patterns and restored capacity for psychological wellbeing.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Depressed, Suicidal and/or Major Depressive Disorder
This could be your breakthrough. Let's do this!
Depression is not a deficit of willpower. It is a hijacked reward system screaming for recalibration. Major Depressive Disorder (MDD) is a serious mental health condition characterized by persistent feelings of hopelessness, loss of interest in activities, and a pervasive sense of emptiness affecting functioning across all life domains. Individuals with MDD often experience changes in sleep, appetite, and energy levels, along with difficulty concentrating and making decisions. These symptoms can range from mild to severe, and when coupled with suicidal ideation, this condition becomes a serious public health concern requiring immediate intervention.
The neurobiological mechanism underlying depression involves a cascade initiated by chronic anxiety. Chronic anxiety keeps the limbic system in a state of alarm that eventually depletes critical neurotransmitters like serotonin, dopamine, and norepinephrine. This neurochemical depletion leads to the neurobiological 'shut down' state characteristic of clinical depression, where the brain's reward and motivation systems become increasingly suppressed. Over time, this creates a self-reinforcing cycle where the depressed state itself prevents engagement with activities that could naturally elevate mood.
Our technique targets and rewires this cascade through creative reprogramming of the limbic system's reward architecture. We identify the limiting beliefs and amygdala hijacks that trigger the anxiety-depletion cycle, then replace them with new neural patterns of agency and vitality. This is not therapy or talk about your past. It is precision recalibration of the neurochemical systems that have been locked in shutdown mode. You access restored capacity for motivation, pleasure, and will often within sessions.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Major Depressive Disorder - Avolition & Depressive Apathy (Sloth)
This could be your breakthrough. Let's do this!
Your nervous system learned that effort is futile and the future holds nothing worth pursuing. Depression isn't sadness—it's the neurological shutdown where motivation ceases and the world becomes colorless and empty. Major Depressive Disorder (MDD) is characterized by persistent low mood, loss of interest or pleasure in activities (anhedonia), significant appetite or weight changes, sleep disturbance, fatigue and loss of energy, feelings of worthlessness or guilt, difficulty concentrating, and recurrent thoughts of death. In depressive apathy (sometimes called "sloth"), the defining feature is avolition—the complete absence of motivation to initiate any directed behavior, not because the person is lazy but because the brain's motivation systems have shut down entirely. Severely depressed individuals report that even breathing feels like too much effort.
The neurobiological mechanism involves widespread dysregulation of the brain's reward, motivation, and energy systems. The nucleus accumbens (reward processing and motivation generation) shows reduced dopamine activity—anticipated rewards no longer generate motivational pull. The ventromedial prefrontal cortex becomes hyperactive in negative rumination and hopelessness prediction but fails to activate with positively-oriented future-thinking. The dorsolateral prefrontal cortex loses capacity for goal-directed planning and cognitive control. The anterior cingulate cortex becomes dysregulated in error-detection, generating persistent self-criticism ("Everything I do is wrong"). The amygdala becomes hyperresponsive to loss and threat while the insula generates persistent distress signals that the brain interprets as "this situation is intolerable." Sleep architecture becomes disrupted (reduced REM latency, fragmented sleep), perpetuating fatigue. The hypothalamic-pituitary-adrenal (HPA) axis remains chronically activated, generating cortisol that further damages motivation and cognitive function. The person's brain has literally lost the capacity to generate the neurochemical reward and motivation necessary to initiate behavior. This isn't weakness or laziness—it's a brain in neurological shutdown.
Our technique restores dopamine signaling in the nucleus accumbens and rebuilds the brain's capacity to generate motivation and reward-anticipation. We recalibrate the ventromedial prefrontal cortex's hopelessness and restore access to genuine future-oriented thinking. The dorsolateral prefrontal cortex regains capacity for goal-directed planning. We recalibrate the HPA axis hyperactivity and restore normal stress-response patterns. The amygdala becomes less hyperresponsive to loss and threat. The brain's energy systems recalibrate—fatigue decreases and the person regains capacity to initiate directed behavior. Sleep architecture normalizes. The anhedonia resolves as the nucleus accumbens relearns to generate reward and motivation. You experience restored ability to experience pleasure, return of genuine motivation and goal-directed behavior, decreased fatigue where effort becomes possible again, hopeful future-orientation, and the restoration of the will-to-live where the world becomes colorful again and the future feels worth pursuing.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.BPD - Bipolar Disorder
This could be your breakthrough. Let's do this!
Your mood system is a pendulum that's swinging too far. It's time to find the center. Bipolar Disorder is a mood disorder characterized by alternating episodes of depression and mania (or hypomania in Bipolar II), with periods of normal mood in between or varying states of mixed mood. During manic episodes, individuals experience decreased need for sleep, racing thoughts, increased goal-directed activity, and impaired judgment that can lead to risky behaviors and damaged relationships. During depressive episodes, individuals experience the full constellation of depressive symptoms described earlier, often with particularly severe suicidality.
The neurobiological underpinnings of Bipolar Disorder involve dysregulation of circadian rhythms, neurotransmitter systems, and the neural networks governing mood stability. Stress and anxiety act as primary destabilizers for these already-fragile systems, frequently acting as the catalyst for a shift into mania, a depressive crash, or a mixed-affective state where depression and mania coexist simultaneously. High stress periods often correlate with mood episode onset, suggesting that managing stress and anxiety may be crucial to mood stability. The amygdala's threat perception directly influences the balance between sympathetic arousal and parasympathetic calm.
Our technique stabilizes the nervous system's stress response patterns through targeted recalibration of limbic reactivity. We restore rhythm to the circadian and neurotransmitter systems by reducing chronic anxiety and improving the brain's capacity to maintain equilibrium under stress. This isn't just medication adjustment or lifestyle counseling. It's targeted recoding of the threat-detection and mood-regulation systems. Many participants experience increased intervals between mood episodes, reduced severity of episodes, and newfound stability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Hyper Cynicism - Depressive Realism, Pervasive Distrust & Defensive Negativity
This could be your breakthrough. Let's do this!
Your nervous system may have decided that hope is what gets people hurt. Hyper cynicism is not ordinary skepticism or healthy discernment. It is a rigid, overlearned interpretive stance in which the mind narrates people, systems, motives, and future outcomes through a lens of betrayal, futility, corruption, or inevitable disappointment. The person may feel that they are simply being "realistic" while everyone else is naive, sentimental, or self-deceived. In some individuals this resembles what has been called depressive realism: a stark, linear, bias-stripped view of life in which optimism feels dishonest and cynicism feels like truth. In more severe or personality-structured forms it can overlap with pervasive distrust, including paranoid predictions of betrayal or harm, or schizoid-style detachment where cynicism functions as a defensive wall against the vulnerability of social connection. This stance is often a compensation for the opposite pole: when defensive idealization, wish-based thinking, or naive trust has previously exposed the person to humiliation, exploitation, betrayal, or moral injury, the mind may swing into hyper cynicism to make sure openness never becomes that dangerous again. In workplace variants, the same stance gets projected onto employers, leadership, missions, customers, or the entire concept of meaningful work, especially after chronic overextension, hypocrisy exposure, or repeated exploitation. In relationship variants, the nervous system may begin treating intimacy itself as a setup for disappointment, using sarcasm, suspicion, emotional distance, or preemptive contempt to avoid dependence, grief, or humiliation. It is also common in occupational burnout, where chronic overtaxing leads to emotional distance, negativism, and contempt for the entire work system, and in moral injury, where the person begins to interpret future people and institutions through a hardened lens designed to prevent ever being fooled or violated again.
The neurobiological mechanism involves chronic threat-based prediction dominating interpretation. The amygdala and salience systems bias attention toward evidence of danger, hypocrisy, incompetence, betrayal, or collapse. The anterior cingulate cortex remains over-engaged in error-detection and contradiction-monitoring, constantly scanning for what is wrong or unsafe. The ventromedial prefrontal cortex develops hardened beliefs such as "people always disappoint," "systems are rigged," "every relationship ends in betrayal," or "hope is for fools," and then uses those beliefs to interpret new information before it is fully evaluated. The dorsolateral prefrontal cortex may construct elaborate justifications for the cynical stance, making it feel intellectually superior rather than emotionally defended. The insula tags interpersonal contact, institutions, work obligations, and future-oriented thinking with disgust, dread, or deadness rather than curiosity or possibility. In many cases this is a compensatory correction against a prior history of overtrust, idealization, or denial: the nervous system learns that if it expects the worst, it cannot be fooled in the same way again. In burnout, the PFC narrates chronic limbic exhaustion as the uselessness of the work, the mission, or the people involved. In relationship-focused variants, attachment cues themselves become fused with anticipated disappointment, engulfment, betrayal, or ridicule, so distance starts feeling safer than tenderness. In moral injury, future trust is filtered through the memory of value-violation so the organism is never caught undefended again. What looks like philosophical realism is often a nervous system that no longer feels safe enough to generate openness, trust, or adaptive optimism.
Our technique targets the threat-prediction machinery beneath the cynical narrative. We recalibrate the amygdala's reflexive expectation of betrayal, restore flexibility to the ventromedial prefrontal cortex's world-models, and reduce the anterior cingulate's compulsive fixation on what's wrong, corrupt, or doomed. We help the insula distinguish true danger from habituated negativism and re-open access to social, relational, vocational, and existential engagement without forcing fake positivity. This is not an attempt to make someone gullible, compliant, or blind to genuine corruption. It is the restoration of discernment without totalized distrust. You experience less compulsive negativism, reduced need to protect yourself through contempt or emotional distance, greater capacity to evaluate people, work systems, and intimate relationships realistically without collapsing into bitterness, and a nervous system that no longer mistakes openness for danger or cynicism for truth itself.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Defensive Idealization - Unrealistic Optimism, Reality Avoidance & Wish-Based Thinking
This could be your breakthrough. Let's do this!
Your nervous system may have decided that the only tolerable future is the one it beautifies, sanitizes, or spiritually guarantees. Defensive idealization is the opposite pole of hyper cynicism. Instead of anticipating betrayal, collapse, or disappointment, the mind overcorrects toward unrealistic optimism, selective attention to reassuring signs, and a refusal to metabolize contradictory evidence. This is not grounded hope, resilience, or mature faith. It is an overlearned protective style in which danger gets minimized, motives get idealized, and complexity gets replaced with certainty that "everything will work out" if one just stays positive, trusts hard enough, or refuses to look directly at what is happening. In some individuals it appears as chronic denial, in others as relational idealization, redemptive certainty, suggestibility to charismatic personalities, or wish-based thinking that treats desire as evidence. This stance is often a compensation for the opposite pole: when hyper cynicism, chronic distrust, or repeated anticipation of betrayal has become unbearable, the mind may swing toward idealization, magical reassurance, and naive faith because certainty feels safer than living in permanent suspicion. This can create unusual vulnerability to narcissists, conmen, manipulative gurus, apocalyptic belief systems, superstition, and rigid religiosity, because the person's need for reassurance outruns their reality-testing. In more spiritualized forms it can resemble spiritual bypassing, where grief, anger, accountability, and skepticism are skipped in favor of destiny narratives, miraculous explanations, prophetic certainty, or the conviction that discernment itself is a lower form of consciousness.
The neurobiological mechanism involves top-down inhibition of threat information rather than healthy integration of it. The ventromedial prefrontal cortex generates overly coherent positive narratives that suppress disconfirming evidence before it can fully update the model of reality. The anterior cingulate cortex becomes less willing to sustain contradiction, ambiguity, or error-signals, so the person exits uncertainty too quickly and lands in premature reassurance. The dorsolateral prefrontal cortex may become recruited into rationalization, constructing polished explanations for why obvious risks do not apply, why boundaries are unnecessary, why a charismatic person must be trustworthy, or why improbable claims should be accepted because they feel meaningful. The amygdala's warnings may be chronically bypassed, numbed, or reinterpreted as mere negativity rather than useful data. The insula's uncomfortable signals of dread, aversion, or intuition are overruled by a learned mandate to stay uplifted, surrendered, faithful, or certain. In many cases this is a compensatory correction against a prior state of bitterness, suspicion, or collapse into distrust: the nervous system reaches for idealization because unbuffered cynicism feels intolerable. In relationship variants, it can appear as idealizing unavailable, exploitative, or grandiose partners, dismissing red flags as tests of love or faith, and repeatedly converting manipulation into a redemption story. In spiritual or superstitious variants, coincidence gets over-read as destiny, authority gets confused with wisdom, and the need for cosmic safety can override evidence, boundaries, and independent judgment. What looks like positivity is often a nervous system that cannot yet tolerate grief, disillusionment, uncertainty, or the pain of seeing clearly.
Our technique restores contact with reality without collapsing the person into despair or cynicism. We help the nervous system tolerate ambiguity, loss, and contradiction so optimism no longer has to be inflated into denial. We recalibrate the ventromedial prefrontal cortex's need for redemptive certainty, strengthen the anterior cingulate's capacity to stay with disconfirming evidence, and restore the insula's role as a source of valid internal warning rather than something to override with affirmations, prophecy, or charm. This is not an attack on hope, meaning, spirituality, or genuine faith. It is the restoration of grounded hope that can face facts. You experience less compulsive idealization, reduced susceptibility to manipulators and grandiose personalities, greater ability to distinguish trust from fantasy and reverence from submission, clearer perception of red flags without collapsing into paranoia, and a nervous system that no longer mistakes denial for faith or wish-based thinking for wisdom.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Seasonal Affective Disorder (SAD)
This could be your breakthrough. Let's do this!
Winter darkness triggers your nervous system into a depressive shutdown that feels involuntary because it is—until recalibration. Seasonal Affective Disorder is a type of depression triggered by seasonal changes, typically beginning in fall or early winter and remitting in spring or summer. Individuals with SAD experience depressed mood, loss of interest in activities, increased sleep, appetite changes, and profound fatigue during specific seasons, often causing occupational and social dysfunction during winter months which then resolves when seasons change.
The neurobiological mechanism involves dysregulation of circadian rhythms caused by reduced light exposure during winter months. Lower light levels suppress melatonin regulation and serotonin production, leading to depressed mood and fatigue. The suprachiasmatic nucleus fails to maintain robust circadian signaling, disrupting sleep-wake cycles and dopamine-driven motivation. The prefrontal cortex becomes increasingly hypofunctional as serotonin declines, reducing capacity for effortful engagement and mood regulation. Additionally, the amygdala may become sensitized to seasonal darkness as a threat signal, triggering depressive shutdown as a false protective response.
Our technique recalibrates circadian rhythm sensitivity to seasonal light changes through targeted limbic intervention. We restore robust dopamine and serotonin signaling independent of seasonal darkness. Your nervous system ceases to treat winter darkness as threat or signal for depressive shutdown. You experience consistent mood and motivation year-round without seasonal variation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Perinatal & Postpartum Depression
This could be your breakthrough. Let's do this!
Pregnancy and birth triggered a nervous system crash. The neurobiological upheaval of perinatal/postpartum transition created depressive shutdown. Perinatal and postpartum depression encompasses depression during pregnancy (perinatal) or following childbirth (postpartum), characterized by depressed mood, loss of interest in the baby, guilt, worthlessness, thoughts of harm, and severe functional impairment. This differs from "baby blues" in intensity and duration, and without treatment causes profound suffering during what should be bonding and attachment periods.
The neurobiological mechanism involves massive hormonal shifts—particularly sharp drops in estrogen and progesterone post-delivery—that dysregulate neurotransmitter systems including serotonin, dopamine, and GABA. The hippocampus becomes hypofunctional due to cortisol elevation from birth stress, impairing memory and learning of infant cues. Sleep deprivation from newborn care further dysregulates limbic systems and impairs prefrontal function. The amygdala may become sensitized to infant distress sounds as threat, creating anxiety and avoidance rather than bonding. Socially-conditioned expectations of instant maternal bonding create additional shame when depression prevents affective engagement.
Our technique recalibrates the nervous system's response to perinatal hormonal and sleep shifts through targeted limbic and endocrine intervention. We restore monoamine signaling and hippocampal function independent of hormonal status. Your nervous system regains capacity for bonding, pleasure, and engagement with your baby and life. You experience freedom from perinatal/postpartum depression and access to genuine maternal (or paternal) connection.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Menopausal Depression
This could be your breakthrough. Let's do this!
Your nervous system crashed when estrogen declined. Menopause altered the neurochemical foundation that monoamine systems depend on. Menopausal depression is depression triggered or exacerbated during the menopausal transition or postmenopausal period, characterized by depressed mood, loss of interest, fatigue, cognitive changes, and often co-occurring anxiety and sleep disruption. This occurs specifically during hormonal transition and may represent an individual's first depressive episode or reactivation of previous depression.
The neurobiological mechanism involves the dramatic decline in estrogen during menopause, which serves as a neuromodulator supporting serotonin and dopamine systems. As estrogen drops, serotonin and dopamine become dysregulated, leading to depression and anhedonia. The noradrenergic system becomes hyperactive as compensatory response, creating anxiety and sleep disruption. The hippocampus becomes more vulnerable to stress-induced atrophy during menopause, impairing memory and emotional regulation. Additionally, hot flashes, night sweats, and sleep deprivation from these symptoms further dysregulate the nervous system. The amygdala may become sensitized to menopause-related bodily sensations as threat.
Our technique recalibrates monoamine systems and limbic sensitivity to menopausal hormonal and physical changes through targeted intervention. We restore neurochemical balance independent of estrogen levels and recalibrate threat-sensitivity to menopause-related sensations. Your nervous system regains capacity for mood stability, motivation, and engagement. You experience freedom from menopausal depression and restored quality of life during and after menopause.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Geriatric Depression - Late-Life Mood Dysregulation
This could be your breakthrough. Let's do this!
Your nervous system is processing the cumulative losses of aging—loss of function, loss of independence, loss of friends and peers, loss of identity as a productive person—and the depression is your body's way of adapting to a future it did not plan for. Geriatric Depression or Late-Life Depression occurs primarily in older adults (typically 65+) and is characterized by persistent depressed mood, loss of interest in activities, changes in appetite and sleep, fatigue, difficulty concentrating, feelings of worthlessness, and often suicidal ideation. Unlike depression in younger populations that may seem reactive to specific stressors, geriatric depression often occurs in the context of cumulative losses, chronic medical illness, medication side effects, social isolation, and existential awareness of mortality.
The neurobiological mechanism involves multiple overlapping systems dysregulation: the monoamine systems (serotonin, dopamine, norepinephrine) show age-related decline exacerbated by depression; the hypothalamic-pituitary-adrenal (HPA) axis becomes dysregulated with chronic stress and aging, maintaining elevated cortisol that erodes hippocampal volume and mood-regulation; the prefrontal cortex shows reduced glucose metabolism and connectivity; neuroinflammation increases with age and is associated with depression; the nucleus accumbens shows reduced dopamine responsiveness, making activities that once brought joy no longer rewarding. Brain-derived neurotrophic factor (BDNF) declines with age and depression, reducing neuroplasticity. Chronic medical illnesses (stroke, Parkinson's, cardiovascular disease) create specific damage to mood-regulation circuitry. Medications for other conditions (corticosteroids, beta-blockers, anticholinergics) can worsen depression. Social isolation reduces the environmental stimulation needed to maintain dopamine and reduce rumination.
Our technique addresses the multiple biological vulnerabilities of late-life depression by supporting neuroplasticity despite age-related decline, recalibrating the HPA axis through stress-reduction and cortisol-management, activating dopamine pathways through meaningful engagement and social connection, and addressing existential aspects of aging through meaning-making rather than denial. We help the person integrate losses while discovering renewed purpose. Medical optimization (medication review, treatment of underlying conditions) combines with limbic recalibration. You experience improved mood and energy, restored interest in activities and relationships, reduced existential despair, improved sense of meaning and purpose in the later chapters of life, and prevention of the isolation that worsens geriatric depression.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Self-Esteem & Identity Issues
This could be your breakthrough. Let's do this!
Your self-perception became distorted by false threat assessments about your worth. The neural encoding of self became corrupted. Self-esteem and identity issues involve chronic negative self-perception, feelings of unworthiness or inadequacy, persistent self-criticism, difficulty claiming personal accomplishments, and core identity confusion about who "I really am." Individuals with self-esteem issues often feel fundamentally flawed despite evidence of competence or positive qualities, leading to perfectionism, social withdrawal, underachievement, or compensatory overachievement driven by proving worth.
The neurobiological mechanism involves the medial prefrontal cortex—which encodes self-representation and identity—incorporating threat-based or shame-based encoding of self-worth. The amygdala becomes hypersensitive to threat to reputation, status, or competence, treating any criticism or failure as profound identity threat. The anterior cingulate cortex generates persistent self-critical rumination that reinforces negative self-encoding. The default mode network becomes overactive in internally-focused self-evaluation, especially when threat-activated. Social threat becomes encoded as self-threat, and the self-representation becomes fundamentally distorted toward inadequacy.
Our technique recalibrates the self-representation in the medial prefrontal cortex and reduces amygdala's sensitivity to status/competence threat through targeted identity and limbic intervention. We restore accurate self-perception free from threat-distortion. Your nervous system encodes self-worth based on authentic capability and intrinsic value. You experience stable healthy self-esteem and clarified authentic identity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Imposter Syndrome
This could be your breakthrough. Let's do this!
Your nervous system adopted a false belief: that your success is fraudulent and exposure is inevitable. It's time to restore accurate self-assessment. Imposter syndrome is characterized by persistent self-doubt, feelings of fraudulence despite objective evidence of competence and accomplishment, and anxiety that one will be 'exposed' as inadequate. Individuals with imposter syndrome attribute success to external factors (luck, timing, others' help) while internalizing failure as confirmation of inadequacy. This creates a state of perpetual anxiety about being 'found out,' leading to over-preparation, perfectionism, difficulty accepting praise, and underutilization of capabilities. Imposter syndrome is extremely common, particularly among high-achievers, women, and marginalized populations.
The neurobiological mechanism involves a systematic bias in threat-detection where the amygdala hypervigilantly monitors for evidence of inadequacy while minimizing evidence of competence. The prefrontal cortex becomes hijacked by catastrophic narratives about exposure and public failure. When accomplishments occur, the brain's reward system becomes suppressed—the amygdala treats success as danger (it increases visibility and exposure risk). This creates a perverse incentive structure where the nervous system paradoxically learns to fear success and competence-visibility. The neural networks encoding self-worth become dysregulated.
Our technique recalibrates the threat-detection bias and restores accurate self-assessment through targeted limbic recalibration. We dissolve the hypervigilance to exposure threat and restore amygdala regulation when processing genuine accomplishments. You experience restored confidence in genuine competence, reduced anxiety about being 'found out,' and authentic pride in accomplishments. This isn't affirmation or confidence building. It's recoding of how your nervous system detects threat in success and visibility. You access genuine self-assurance based on accurate neural processing of your actual capabilities.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Affluenza & Wealth Integration Gap - Sudden Wealth, Identity Loss & Loss of Purpose
This could be your breakthrough. Let's do this!
Your nervous system spent 40 years organized around one primary mission—survival, accumulation, achievement—and now that the mission is complete, you face an existential void. Affluenza (informal term, though the underlying condition is real) and the wealth integration gap occurs when an individual achieves total financial security or experiences sudden significant wealth increase, and paradoxically experiences a crisis of purpose, motivation, and identity. The person may have achieved financial security through inheritance, business success, lottery, or years of accumulation, and now confronts the collapse of their primary life-organizing principle. The survival-drive that provided direction for decades has been satisfied, but the nervous system has not be recalibrated to generate motivation from anything else. Common presentations include depression, identity confusion ("Who am I if I'm not striving?"), loss of meaning and engagement, relationship disruption (partners who provided support during the struggle become unnecessary), behavioral dysregulation (substance use, compulsive spending, infidelity, reckless behavior), or a kind of existential paralysis where the person feels simultaneously freed and trapped.
The neurobiological mechanism involves the collapse of the default-mode network's organizing narrative. For decades, the ventromedial prefrontal cortex has been organized around the computation "my life meaning comes from accumulation/survival" and the anterior cingulate has been hyperactive in effort-allocation around financial goals. The nucleus accumbens became dopamine-responsive to markers of financial progress—each achievement generated reward-surge. When the goal suddenly becomes unnecessary (financial security is complete), the entire reward-system baseline collapses. The person experiences anhedonia (inability to feel pleasure from normal activities) because the nucleus accumbens has been exclusively dopamine-trained to the specific goal that is now irrelevant. The medial prefrontal cortex lacks alternate sources of identity and meaning because 40 years of cognitive resources were devoted to a single mission. The amygdala may paradoxically become hyperactive—sudden wealth often brings new threats (managing investments, family dynamics around inheritance, target for exploitation) that generate ongoing threat-response. The ventromedial prefrontal cortex's value-computation has not been reconsidered to include newer life priorities (relationships, contribution, creativity, learning, legacy) and so these domains fail to generate genuine motivation. The posterior cingulate cortex (autobiographical identity) becomes dysregulated when the person cannot integrate "I am secure and purposeless" into a coherent identity narrative.
Our technique reinstalls the organizing narrative and purpose-generating systems of the nervous system with genuine values-alignment rather than mere survival-drive. We help the medial prefrontal cortex develop coherent identity and life-meaning independent of financial status or accumulation. We reprogram the nucleus accumbens to discover dopamine-reward in genuine contribution, relationships, learning, creative expression, and legacy-building rather than exclusive focus on financial markers. We recalibrate the anterior cingulate to generate effort-allocation for authentic goals rather than only financial accumulation. We help the amygdala recalibrate to distinguish between genuine threats and new trigger-points related to wealth management. We address the ventromedial prefrontal cortex's value-hierarchy to integrate multiple sources of meaning and motivation. We help the person grieve the loss of the driven-identity while building authentic second-act purpose. You experience restoration of genuine motivation and engagement with life-domains beyond financial security, clarified values and purposes independent of accumulation, sustainable meaning-making and identity rooted in contribution and connection, improved relationships based on genuine mutual choice rather than role-based necessity, and the capacity to enjoy financial security as foundation for purposeful living rather than as end-point that creates meaninglessness.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Body Dysmorphia - Distorted Self-Image and Appearance Preoccupation
This could be your breakthrough. Let's do this!
Your nervous system created a distorted map of your appearance and treats it as threat to social acceptability. It's time to restore accurate self-perception. Body dysmorphic disorder (BDD) is characterized by preoccupation with perceived defects in physical appearance that are not observable or appear trivial to others, leading to repetitive behaviors (mirror checking, excessive grooming, skin-picking, reassurance-seeking) and significant distress and functional impairment. Individuals with BDD spend hours preoccupied with appearance flaws, avoid social situations due to perceived unattractiveness, and often pursue cosmetic interventions that provide no relief—because the core issue is the nervous system's distorted threat-perception, not actual appearance defects.
The neurobiological mechanism involves dysfunction in how the visual cortex processes facial features combined with amygdala hyperactivity in response to perceived appearance threat. Brain imaging shows that individuals with BDD have atypical visual processing of faces—focusing on minute details rather than holistic appearance—creating a distorted mental representation. The amygdala treats perceived appearance defects as social threat that threatens belonging and status. Body-checking and reassurance-seeking provide temporary anxiety reduction but reinforce the perception that appearance is a genuine threat. The ventromedial prefrontal cortex fails to regulate the amygdala's threat interpretation of appearance-related stimuli.
Our technique recalibrates appearance-threat perception and restores accurate self-perception through targeted limbic recalibration. We dissolve the amygdala's hyperactivity in response to perceived appearance flaws and restore visual integration. You experience restored accurate perception of your appearance without the threat-based anxiety amplification. Preoccupation recedes as your nervous system stops treating appearance as a genuine social threat. This isn't affirmation or self-esteem work. It's recoding of how your nervous system perceives and encodes appearance threat. You access freedom from appearance preoccupation and authentic social presence.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Eating Disorders - Anorexia, Bulimia, and Binge Eating
This could be your breakthrough. Let's do this!
Food became both control and threat, and your nervous system uses it to manage impossible internal states. It's time to restore genuine nourishment and regulation. Eating disorders (anorexia nervosa, bulimia nervosa, binge eating disorder, and other specified feeding/eating disorder) are serious psychiatric conditions characterized by disturbances in eating behaviors and related thoughts and emotions, leading to significant medical consequences, malnutrition, mortality risk, and severe psychological distress. Individuals with eating disorders use food restriction, purging, or binge-eating to manage anxiety, trauma, perfectionism, control-seeking, or dissociation. The eating disorder provides temporary anxiety regulation but creates severe health consequences including cardiac dysfunction, electrolyte imbalances, lost bone density, and death. Binge eating disorder in particular frequently leads to obesity and weight dysregulation, creating compound medical consequences of both obesity-related disease and the psychological devastation of eating disorder pathology.
The neurobiological mechanism involves amygdala hyperactivity combined with a loss of interoceptive awareness (the ability to sense internal bodily states like hunger/fullness). The insula becomes dysregulated, preventing accurate registration of hunger and satiety signals. Anxiety or emotional distress becomes mis-interpreted as physical hunger or, conversely, blocked from accessing hunger signals entirely. The nervous system uses food control/restriction or binge episodes to downregulate anxiety/trauma through temporary neurochemical shifts. Perfectionism-driven restrictive eating activates reward pathways, creating a pleasurable sense of control that reinforces restriction. The orbitofrontal cortex becomes hyperactive in habit-formation around eating behaviors. The neural circuits encoding safety, nourishment, and self-care become corrupted.
Our technique recalibrates anxiety-management and restores genuine interoceptive awareness through targeted limbic intervention. We dissolve the amygdala hijack that drives restrictive/binge behaviors and restore accurate hunger/fullness signaling. Your nervous system regains capacity to use food for genuine nourishment rather than anxiety-regulation. This isn't nutrition education or cognitive-behavioral techniques. It's recoding of how your nervous system uses food and body control to manage threat and anxiety. You experience restored capacity for balanced eating, body trust, and genuine nourishment.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Addictions & Compulsive Behaviors
General Addictions
This could be your breakthrough. Let's do this!
Your reward system learned to pursue a substance or behavior compulsively despite catastrophic consequences. Addiction patterns vary but the underlying mechanism is consistent: dopamine dysregulation and loss of inhibitory control. Other addictions beyond the primary patterns include shopping addiction, exercise addiction, work addiction, relationship addiction, and diverse compulsive behaviors that individuals pursue despite knowing they cause harm. Each addiction provides temporary dopamine elevation and escape from distress, followed by shame and escalating distress that drives continued pursuit.
The neurobiological mechanism involves dysregulation of the mesolimbic dopamine pathway where the addictive stimulus triggers supernormal dopamine release. The ventromedial prefrontal cortex loses regulatory capacity to inhibit the addictive behavior. The amygdala becomes conditioned to emotional distress (anxiety, boredom, sadness) as a cue to engage the addictive behavior for relief. The anterior cingulate cortex generates compulsive approach toward the addictive target. Regardless of specific addiction, all involve the same core dysregulation: excessive dopamine reward signal combined with loss of executive inhibition and emotional-behavior coupling.
Our technique recalibrates the dopamine reward system and restores executive capacity through targeted limbic intervention. We dissolve the distress-addiction link and restore genuine distress tolerance. Your nervous system ceases pursuing the addictive behavior and accesses genuine satisfaction and emotional regulation alternatives. You experience freedom from addiction and restored capacity for meaningful engagement with life.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Screen Addiction & Digital Escapism - Adolescent Internet Dependence
This could be your breakthrough. Let's do this!
Your adolescent discovered a parallel universe where they are more attractive, more skilled, more powerful, and never have to experience failure or rejection in the way their real body requires. Teen screen addiction and digital escapism occur when an adolescent becomes neurologically dependent on digital stimulation as the primary escape from the intensity and dysregulation of adolescent experience. Screen time provides: endless dopamine-hits from social validation (likes, comments, followers), escapism from real-world social anxiety and failure, identity experimentation in digital personas, and constant stimulation that prevents the boredom and emptiness of the real-world depressed mood. The adolescent's prefrontal cortex becomes unable to engage with real-world challenges because the digital reward-system is supernormally potent. Sleep deteriorates. Real-world relationships become secondary. Academic function declines. The adolescent experiences profound emptiness in non-screen time.
The neurobiological mechanism: social media has been engineered to trigger maximal dopamine-reward in the nucleus accumbens (variable reward schedules = maximum addiction). The adolescent brain's nucleus accumbens is already hypersensitive to reward. The prefrontal cortex is still developing inhibitory capacity and cannot resist the engineered supernormal-stimulus. The anterior insula becomes dysregulated by the constant social comparison (Instagram showing others' highlight reels creates insula-generated feeling of personal inadequacy). The ventromedial prefrontal cortex's sense of self becomes contingent on digital validation (how many likes did I get?). Real-world distress (academic challenges, social anxiety, family conflict) becomes unbearable when compared to the digital-dopamine availability. The sleep system becomes disrupted by blue-light and endless stimulation. The amygdala remains dysregulated because screen-escapism prevents development of genuine distress-tolerance.
Our technique rebuilds dopamine-system baseline so that real-world experiences feel rewarding again (this requires gradual screen reduction, not sudden cessation, because cessation generates withdrawal). The ventromedial prefrontal cortex rebuilds intrinsic self-worth independent of digital validation. The prefrontal cortex regains capacity for inhibitory control around screens. The insula recalibrates to manage real-world social comparison without generating shame. Real-world relationships become sources of dopamine-reward again. The sleep system resets. The adolescent develops capacity for genuine engagement with real-world challenges, experiences, and relationships, rather than constant digital-escapism.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Alcohol and Substance Abuse Disorders
This could be your breakthrough. Let's do this!
Your brain learned that the substance was the answer to an impossible question your nervous system kept asking. Substance Use Disorder is a chronic brain condition characterized by compulsive engagement in drug or alcohol use despite significant negative consequences, including health problems, damaged relationships, employment loss, and legal issues. Addiction hijacks the brain's reward, motivation, and decision-making systems, making it extremely difficult for individuals to stop using substances even when they want to and understand the harm caused. Recovery from addiction is a long-term process requiring comprehensive support, as the brain has become fundamentally rewired around substance use.
Anxiety plays a critical role in the initiation and maintenance of substance addiction—many individuals with anxiety disorder initially turn to substances as a form of self-medication to reduce their overwhelming internal distress. Anxiety creates a state of physiological 'dis~ease' that drives the limbic system to seek immediate relief through dopamine-reward pathways, frequently triggering cravings and relapse. Over time, avoidance of withdrawal symptoms, environmental triggers, and anxiety about not having access to the substance becomes a powerful maintenance factor for continued use. The substance becomes wired into the threat-avoidance system.
Our technique targets the anxiety infrastructure underlying addiction by recalibrating the reward system and threat-detection network. We reprogram the amygdala's anxious alarm that was being 'solved' by substance use and restore the brain's genuine capacity for natural dopamine release and self-regulation. This isn't 12-step programs or behavioral conditioning. It's recoding of the neurological loop that made substances seem necessary. You access genuine recovery where cravings recede and the emotional need for substances dissolves.
Related condition: For adolescent substance abuse during critical developmental windows with different treatment considerations, see Teen Substance Abuse & Addiction.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Teen Substance Abuse & Addiction - Adolescent Chemical Dependence
This could be your breakthrough. Let's do this!
Your adolescent's developing prefrontal cortex discovered that chemicals can solve the unsolvable adolescent nervous system dysregulation—social anxiety, family pain, identity confusion, academic pressure, all evaporates with a single substance. Teen substance abuse and addiction occur when an adolescent's still-developing nervous system becomes chemically dependent before it ever develops genuine emotional regulation capacity. The adolescent may begin substance use as recreation or stress-relief but quickly becomes dependent because the adolescent brain is uniquely vulnerable: the nucleus accumbens is hypersensitive to dopamine (reward-learning is at peak sensitivity), the prefrontal cortex is still under construction (judgment and inhibition are still developing), and the amygdala is threat-reactive and anxious (substances provide immediate relief). Adolescent addiction typically involves the teen hiding use from parents/school, escalating dose/frequency to maintain the effect, experiencing cognitive decline and memory problems, demonstrating personality changes, and continuing use despite catastrophic consequences.
The neurobiological mechanism: the nucleus accumbens of an adolescent is exquisitely sensitive to dopamine—the substance-induced dopamine surge creates supernormal reward-learning. The mesolimbic pathway (from VTA to nucleus accumbens) becomes rapidly sensitized to substance cues. The prefronta cortex is still pruning irrelevant circuits and myelinating critical pathways—it cannot yet provide sufficient inhibitory control. The amygdala is threat-reactive and substance provides immediate amygdala-quieting relief. The ventromedial prefrontal cortex never develops capacity for emotion-regulation, self-soothing, or distress-tolerance because the chemical solution has been available. Long-term heavy substance use in adolescence can cause permanent damage to prefrontal development and white-matter connectivity.
Our technique begins by stabilizing the acute substance-dependence (often requiring medical intervention) and then rebuilding the underdeveloped prefrontal systems. We help the adolescent's nucleus accumbens recognize non-chemical sources of dopamine-reward. The prefrontal cortex develops genuine inhibitory capacity and rational decision-making. The ventromedial prefrontal cortex learns emotion-regulation, distress-tolerance, and self-worthiness that doesn't depend on chemical alteration. The amygdala stops depending on substances for threat-relief and develops behavioral regulation skills. The adolescent experiences restored cognitive capacity, rebuilt relationships with family/school, freedom from chemical dependence, and genuine development of the emotional/regulation systems that substance use prevented.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Gambling Addiction
This could be your breakthrough. Let's do this!
Your dopamine system learned that gambling provides the highest reward and now pursues it compulsively despite catastrophic consequences. Gambling became self-medication for impossible internal states. Gambling disorder is characterized by persistent, compulsive gambling despite significant negative consequences, loss of control over gambling, and escalating amounts of money and risk-taking. Individuals with gambling addiction experience massive financial losses, relationship destruction, occupational impairment, legal consequences, and yet feel unable to stop despite desperately wanting to. Gambling provides temporary relief from anxiety or depression before rebound distress follows.
The neurobiological mechanism involves profound dysregulation of the mesolimbic dopamine pathway, where gambling-related cues trigger dopamine release that reinforces compulsive seeking despite negative outcomes. The prefrontal cortex loses regulatory capacity, failing to inhibit gambling urges despite intellectual awareness of consequences. The amygdala becomes sensitized to emotional distress (anxiety, depression, boredom) as a trigger for gambling urges. Gambling provides temporary dopamine elevation and relief from distress but leads to guilt, shame, and greater distress, increasing the need to gamble again. The cycle becomes self-perpetuating as only gambling provides relief from the distress gambling creates.
Our technique recalibrates the dopamine reward system and dissolves the distress-gambling link through targeted limbic intervention. We restore executive capacity and genuine distress tolerance. Your nervous system ceases to pursue gambling as relief and accesses genuine anxiety-regulation alternatives. You experience freedom from gambling compulsion and restored financial and emotional stability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Food Addiction
This could be your breakthrough. Let's do this!
Food became your primary coping mechanism for internal distress. Hyperpalatable foods hijacked your reward system. Food addiction involves compulsive eating of highly palatable foods (high sugar, fat, salt) despite negative health consequences, loss of control over eating, and using food as primary emotional regulation mechanism. Individuals with food addiction experience progressive obesity, metabolic dysregulation, health complications (cardiovascular disease, type 2 diabetes, sleep apnea, joint damage), shame, social isolation, and repeated failed dieting attempts. The addiction cycle involves eating for emotional relief, temporary dopamine elevation, guilt and shame at weight gain, and escalating hunger for repeated relief. The neurological mechanism parallels substance addiction—the brain treats hyperpalatable food with the same reward dysregulation as cocaine or alcohol, yet the addict must continue engaging with the addictive substance multiple times daily for survival, making food addiction uniquely difficult to treat
The neurobiological mechanism involves dysregulation of the mesolimbic reward pathway where highly palatable foods trigger excessive dopamine release, creating supernormal reward signals that exceed natural food reward. The prefrontal cortex loses regulatory capacity and cannot inhibit eating urges despite health goals. The amygdala becomes sensitized to emotional distress as a cue for eating. The insula loses interoceptive awareness of true hunger and satiety signals, becoming dysregulated by emotional states instead. Opioid pathways become dysregulated, creating craving for food as primary comfort mechanism. The cycle perpetuates as food provides temporary emotional relief before shame and physical discomfort drive further eating.
Our technique recalibrates the food reward system and restores genuine interoceptive awareness through targeted limbic intervention. We dissolve the emotional-eating link and restore prefrontal regulation. Your nervous system ceases using food as primary emotional management and accesses genuine distress-tolerance alternatives. You experience restored capacity for balanced eating, appropriate appetite regulation, and emotional resilience.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.General OCD-Spectrum Issues
This could be your breakthrough. Let's do this!
Intrusive thoughts or impulses hijacked your nervous system and now your brain treats them as genuine threats requiring compulsive responding. OCD spectrum patterns share the core mechanism of threat-misdetection and compulsion-based regulation. General OCD-spectrum issues include diverse obsessions (about harm, sexuality, identity, morality, contamination, perfection) and related compulsions (checking, seeking reassurance, avoidance, mental rituals, ordering, arranging) that cause significant distress and functional impairment. The distinguishing feature is that the compulsions provide only temporary relief before obsessions resurface, creating cycles of increasing distress.
The neurobiological mechanism involves orbitofrontal cortex hyperactivity in error-detection that generates false threat-signals in response to normal thoughts or situations. The anterior cingulate cortex generates persistent error-checking and uncertainty. The amygdala becomes sensitized to obsession-related triggers, and compulsions provide temporary amygdala downregulation through sense-of-control or ritual completion. The cycle becomes self-perpetuating: obsessive thought generates threat-signal, compulsion provides temporary relief, uncertainty returns because compulsion never proves safety, compulsion must repeat. The neural circuitry becomes stuck in a threat-detection loop that treats uncertainty as requiring behavioral management.
Our technique breaks the obsession-compulsion cycle by recalibrating the error-detection system and reducing amygdala threat-sensitivity through targeted limbic intervention. We restore accurate threat-assessment where obsessions no longer trigger compulsions. Your nervous system ceases generating false threat-signals and regains capacity to tolerate uncertainty. You experience freedom from obsessions and compulsions with dramatically reduced distress.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.OCD - Obsessive-Compulsive Disorder
This could be your breakthrough. Let's do this!
Your brain is stuck in a loop, treating intrusive thoughts as actual threats. It's time to break the circuit. Obsessive-Compulsive Disorder is characterized by persistent intrusive thoughts, images, or urges (obsessions) that cause significant anxiety, followed by repetitive behaviors or mental acts (compulsions) performed to neutralize the anxiety or prevent a feared outcome. OCD can involve almost any theme: contamination, harm, aggression, sexual content. The compulsions can range from hand-washing and checking to mental rituals like counting or reassurance-seeking. Individuals with OCD often recognize the irrationality of their thoughts yet feel unable to stop the compulsive cycles that consume hours of their day.
The neurobiological loop in OCD involves a circuit between the orbitofrontal cortex (involved in error detection and value assignment) and the amygdala (processing threat and fear). This loop creates a cycle where anxiety drives the intense need for compulsions to neutralize perceived threats or manage intrusive thoughts. The compulsion provides temporary relief, negatively reinforcing the obsessive-compulsive pattern and making it progressively more entrenched. Over time, the brain becomes increasingly sensitized to potential threats, leading to expansion of obsessive themes and proliferation of compulsive rituals. The amygdala misclassifies intrusive thoughts as life-threatening.
Our technique breaks the obsessive-compulsive circuit through targeted recalibration of the amygdala-orbitofrontal connection. We dissolve the threat response to intrusive thoughts and restore prefrontal regulation. Intrusive thoughts become less emotionally charged and the compulsive urges recede. This isn't exposure-response prevention or cognitive therapy. It's swift recoding of the threat-detection circuit. You observe obsessive thoughts without the urgent need to engage in compulsions. Daily distress and functioning improve substantially.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Hoarding Disorder
This could be your breakthrough. Let's do this!
Your brain learned that acquiring and keeping possessions reduces anxiety. The neural circuits for decision-making and emotional regulation became hoarding-focused. Hoarding disorder is characterized by excessive accumulation of possessions, difficulty discarding items (regardless of actual value), and significant distress or functional impairment caused by cluttered living spaces. Individuals with hoarding disorder experience decision paralysis when facing item disposal, intense anxiety at the thought of discarding items, and strong attachment to objects that exceeds their functional value. Living spaces become unsafe, unsanitary, or unusable.
The neurobiological mechanism involves amygdala hyperreactivity to the idea of discarding items, where letting go of possessions triggers existential loss threat disproportionate to the item's actual value. The ventromedial prefrontal cortex becomes hyperactive in attribution of too-much-meaning to objects, and loss-aversion becomes pathologically overamplified compared to normal loss-aversion. The dorsolateral prefrontal cortex loses capacity to override these threat and loss-aversion signals through rational decision-making. Items become imbued with emotional significance or hypothetical future utility that prevents discarding. The pattern becomes self-reinforcing as acquisition provides temporary dopamine relief from anxiety, then accumulated items generate anxiety about disposal.
Our technique recalibrates item-meaning attribution and loss-aversion through targeted limbic intervention. We restore appropriate decision-making capacity and realistic meaning assignment to possessions. Your nervous system ceases extracting excessive emotional significance from objects. You experience freedom to make discard decisions and restored capacity to maintain functional living spaces.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Cutting & Self-Harm
This could be your breakthrough. Let's do this!
Your nervous system learned that physical pain provides relief from psychological distress. Self-injury became your primary emotion regulation system. Cutting and self-harm behaviors involve intentional injury to the body (cutting, burning, picking, hitting) as primary mechanism for emotional regulation, dissociation management, or self-punishment. Individuals who self-injure typically experience intense emotional pain, dissociation, or emotional numbness and find that physical pain provides temporary relief or reconnection. The cycle becomes entrenched where emotional distress triggers self-injury, temporary relief follows, then guilt and shame drive escalated need to self-injure again.
The neurobiological mechanism involves dysregulation of pain processing and emotion regulation pathways. When emotional distress becomes intolerable, physical pain signal activates the brain's endogenous opioid system, providing temporary dopamine-based relief and emotional numbness. The amygdala's threat-perception drives emotional distress that becomes unbearable within the current distress-tolerance capacity. The anterior insula loses accurate interoceptive awareness, preventing accurate sensing of emotional state and creating dissociative disconnection. Self-harm provides the bridge that generates physical sensation when emotional sensation becomes unbearable. The pattern becomes self-reinforcing as it successfully provides temporary regulation.
Our technique builds genuine distress tolerance and restores emotional regulation without self-injury through targeted limbic and identity intervention. We dissolve the self-harm to relief link and establish healthier regulation pathways. Your nervous system regains capacity to tolerate intense emotion without requiring physical pain. You experience freedom from urges to self-harm and restored capacity to be present in your body and emotions without medical consequences.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Trichotillomania and Body-Focused Repetitive Behaviors
This could be your breakthrough. Let's do this!
Your nervous system learned to use hair-pulling or skin-picking to self-soothe an anxious threat state. The calming is temporary but the damage is real. Trichotillomania (hair-pulling disorder) and related body-focused repetitive behaviors (BFRBs) like skin-picking, nail-biting, and lip-chewing are characterized by repetitive self-injurious behavior that provides temporary emotional regulation and anxiety relief but results in visible tissue damage, social shame, and significant functional and health consequences. Individuals with BFRBs often engage in these behaviors during stress or boring states, often without conscious awareness, creating dissociative-like trance states. Despite understanding the harm, individuals continue engaging in the behaviors because they provide genuine (though temporary) anxiety-regulation.
The neurobiological mechanism involves a hijacking of the natural repetitive-behavior system (which provides soothing through rhythmic stimulation) to manage anxiety. When anxiety or internal distress emerges, the nervous system learns that hair-pulling or skin-picking produces temporary neurotransmitter-based soothing through endogenous opioid release. This creates a self-medication cycle where anxiety drives the behavior, temporary relief reinforces it, then rebound anxiety and tissue damage follow. The orbitofrontal cortex (involved in habit-formation) becomes hyperactive, the anterior cingulate cortex signals error-detection that escalates anxiety, and the amygdala drives the urge to engage in the BFRB for anxiety relief.
Our technique dissolves the anxiety-BFRB link by recalibrating how the nervous system manages distress and providing genuine anxiety-reduction alternatives. We reprogram the habit loop and restore genuine anxiety-regulation capacity. Urges to engage in self-injurious behaviors recede as the nervous system accesses healthier soothing pathways. This isn't habit replacement or willpower. It's recoding of how your nervous system learned to use self-injury for emotion regulation. You experience freedom from the urge and restored tissue integrity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Food Phobia & ARFID - Phobic Avoidance of Specific Foods
This could be your breakthrough. Let's do this!
Your nervous system learned that certain foods are dangerous, and your brain has locked this assessment into permanent threat-status. Food phobia and Avoidant/Restrictive Food Intake Disorder (ARFID) involve intense fear and avoidance of specific foods based on sensory characteristics (texture, taste, appearance, smell), fear of aversive consequences (choking, vomiting, contamination), or learned negative associations. Unlike eating disorders (where restriction serves anxiety/control management) or food addiction (where specific foods trigger reward dysregulation), ARFID involves genuine phobic response where the amygdala has classified certain foods as threat requiring avoidance. The person often knows the fear is irrational but cannot override it. ARFID frequently begins in childhood with traumatic eating experiences (choking, food-related vomiting, pressure-feeding) and escalates into a severely restricted diet that impairs nutrition and social functioning. The person may eat only 5-10 foods and experience severe anxiety at mealtimes or social eating situations.
The neurobiological mechanism involves amygdala hyperactivity and fear-conditioning around specific food stimuli. The amygdala has learned to treat specific foods as threat-signals requiring escape/avoidance. The insula becomes hyperresponsive to sensory characteristics of the feared foods—a texture becomes intolerable, a taste becomes disgusting, an appearance triggers gagging. This is not a realistic assessment of danger; it's a dysregulated sensory-threat detection where the brain has learned to perceive normal food sensations as aversive or dangerous. The dorsolateral prefrontal cortex cannot override the amygdala's threat assessment despite conscious knowledge that the food is not dangerous. The vagus nerve becomes hyperactive, triggering gagging or nausea in anticipation of the feared food. Previous traumatic experiences (choking, aspiration, food-induced vomiting) have created genuine threat-associations that require targeted limbic intervention to resolve.
Our technique recalibrates the amygdala's threat-classification of the feared foods and helps the insula modulate its dysregulated sensory-response. We carefully work with the person's fear hierarchy, gradually reintroducing feared foods in ways that allow the nervous system to update its threat-assessment. We separate genuine safety concerns (an actual choking risk) from irrational threat-perception. We dissolve the conditioned fear-response through targeted limbic work rather than through exposure alone. You experience expanded food acceptance and dietary diversity, reduced anxiety around mealtimes and social eating, improved nutrition and health, and freedom from the social isolation that ARFID often creates.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Love, Attachment & Couples
Anxious and Avoidant Attachment Patterns
This could be your breakthrough. Let's do this!
Your nervous system learned to approach relationships as either threats to escape or threats to cling to. Authentic connection restores secure integration. Attachment patterns are learned relational strategies established in early caregiving relationships and then generalized to all intimate connections. Anxiously attached individuals experience persistent fear of abandonment, seeking excessive reassurance and becoming hyper-responsive to partner availability. Avoidantly attached individuals experience discomfort with intimacy and closeness, maintaining emotional distance and dismissing relational needs. Both patterns create relationship instability, conflict, and prevent access to genuine secure connection and trust. These patterns often alternate or co-exist, creating chaotic relational dynamics.
The neurobiological mechanism involves early programming of the attachment system where caregiving was either unreliably available (creating anxious hypervigilance to caregiver availability) or invalidating of needs (creating avoidant deactivation of attachment-seeking). These early experiences program the amygdala to perceive closeness as either dangerous (avoidant) or insufficiently available (anxious). The polyvagal complex—which governs relational engagement—becomes dysregulated. Intimate relationships trigger automatic protective patterns where the nervous system either desperately seeks reassurance or defensively withdraws. Genuine rest in another's presence becomes neurologically unavailable.
Our technique reprograms the attachment circuitry by recalibrating the amygdala's perception of intimacy and relational threat. We restore ventral vagal tone—the neurological foundation for safe, connected relationships. Anxious clinging transforms into genuine confidence in connection; avoidant distance transforms into authentic intimacy capacity. This isn't relationship counseling or attachment education. It's recoding of early programming at the nervous system level. You access secure attachment capacity where both closeness and autonomy feel safe.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Hyper Cynicism - Depressive Realism, Pervasive Distrust & Defensive Negativity
This could be your breakthrough. Let's do this!
Your nervous system may have decided that hope is what gets people hurt. Hyper cynicism is not ordinary skepticism or healthy discernment. It is a rigid, overlearned interpretive stance in which the mind narrates people, systems, motives, and future outcomes through a lens of betrayal, futility, corruption, or inevitable disappointment. The person may feel that they are simply being "realistic" while everyone else is naive, sentimental, or self-deceived. In some individuals this resembles what has been called depressive realism: a stark, linear, bias-stripped view of life in which optimism feels dishonest and cynicism feels like truth. In more severe or personality-structured forms it can overlap with pervasive distrust, including paranoid predictions of betrayal or harm, or schizoid-style detachment where cynicism functions as a defensive wall against the vulnerability of social connection. This stance is often a compensation for the opposite pole: when defensive idealization, wish-based thinking, or naive trust has previously exposed the person to humiliation, exploitation, betrayal, or moral injury, the mind may swing into hyper cynicism to make sure openness never becomes that dangerous again. In workplace variants, the same stance gets projected onto employers, leadership, missions, customers, or the entire concept of meaningful work, especially after chronic overextension, hypocrisy exposure, or repeated exploitation. In relationship variants, the nervous system may begin treating intimacy itself as a setup for disappointment, using sarcasm, suspicion, emotional distance, or preemptive contempt to avoid dependence, grief, or humiliation. It is also common in occupational burnout, where chronic overtaxing leads to emotional distance, negativism, and contempt for the entire work system, and in moral injury, where the person begins to interpret future people and institutions through a hardened lens designed to prevent ever being fooled or violated again.
The neurobiological mechanism involves chronic threat-based prediction dominating interpretation. The amygdala and salience systems bias attention toward evidence of danger, hypocrisy, incompetence, betrayal, or collapse. The anterior cingulate cortex remains over-engaged in error-detection and contradiction-monitoring, constantly scanning for what is wrong or unsafe. The ventromedial prefrontal cortex develops hardened beliefs such as "people always disappoint," "systems are rigged," "every relationship ends in betrayal," or "hope is for fools," and then uses those beliefs to interpret new information before it is fully evaluated. The dorsolateral prefrontal cortex may construct elaborate justifications for the cynical stance, making it feel intellectually superior rather than emotionally defended. The insula tags interpersonal contact, institutions, work obligations, and future-oriented thinking with disgust, dread, or deadness rather than curiosity or possibility. In many cases this is a compensatory correction against a prior history of overtrust, idealization, or denial: the nervous system learns that if it expects the worst, it cannot be fooled in the same way again. In burnout, the PFC narrates chronic limbic exhaustion as the uselessness of the work, the mission, or the people involved. In relationship-focused variants, attachment cues themselves become fused with anticipated disappointment, engulfment, betrayal, or ridicule, so distance starts feeling safer than tenderness. In moral injury, future trust is filtered through the memory of value-violation so the organism is never caught undefended again. What looks like philosophical realism is often a nervous system that no longer feels safe enough to generate openness, trust, or adaptive optimism.
Our technique targets the threat-prediction machinery beneath the cynical narrative. We recalibrate the amygdala's reflexive expectation of betrayal, restore flexibility to the ventromedial prefrontal cortex's world-models, and reduce the anterior cingulate's compulsive fixation on what's wrong, corrupt, or doomed. We help the insula distinguish true danger from habituated negativism and re-open access to social, relational, vocational, and existential engagement without forcing fake positivity. This is not an attempt to make someone gullible, compliant, or blind to genuine corruption. It is the restoration of discernment without totalized distrust. You experience less compulsive negativism, reduced need to protect yourself through contempt or emotional distance, greater capacity to evaluate people, work systems, and intimate relationships realistically without collapsing into bitterness, and a nervous system that no longer mistakes openness for danger or cynicism for truth itself.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Defensive Idealization - Unrealistic Optimism, Reality Avoidance & Wish-Based Thinking
This could be your breakthrough. Let's do this!
Your nervous system may have decided that the only tolerable future is the one it beautifies, sanitizes, or spiritually guarantees. Defensive idealization is the opposite pole of hyper cynicism. Instead of anticipating betrayal, collapse, or disappointment, the mind overcorrects toward unrealistic optimism, selective attention to reassuring signs, and a refusal to metabolize contradictory evidence. This is not grounded hope, resilience, or mature faith. It is an overlearned protective style in which danger gets minimized, motives get idealized, and complexity gets replaced with certainty that "everything will work out" if one just stays positive, trusts hard enough, or refuses to look directly at what is happening. In some individuals it appears as chronic denial, in others as relational idealization, redemptive certainty, suggestibility to charismatic personalities, or wish-based thinking that treats desire as evidence. This stance is often a compensation for the opposite pole: when hyper cynicism, chronic distrust, or repeated anticipation of betrayal has become unbearable, the mind may swing toward idealization, magical reassurance, and naive faith because certainty feels safer than living in permanent suspicion. This can create unusual vulnerability to narcissists, conmen, manipulative gurus, apocalyptic belief systems, superstition, and rigid religiosity, because the person's need for reassurance outruns their reality-testing. In more spiritualized forms it can resemble spiritual bypassing, where grief, anger, accountability, and skepticism are skipped in favor of destiny narratives, miraculous explanations, prophetic certainty, or the conviction that discernment itself is a lower form of consciousness.
The neurobiological mechanism involves top-down inhibition of threat information rather than healthy integration of it. The ventromedial prefrontal cortex generates overly coherent positive narratives that suppress disconfirming evidence before it can fully update the model of reality. The anterior cingulate cortex becomes less willing to sustain contradiction, ambiguity, or error-signals, so the person exits uncertainty too quickly and lands in premature reassurance. The dorsolateral prefrontal cortex may become recruited into rationalization, constructing polished explanations for why obvious risks do not apply, why boundaries are unnecessary, why a charismatic person must be trustworthy, or why improbable claims should be accepted because they feel meaningful. The amygdala's warnings may be chronically bypassed, numbed, or reinterpreted as mere negativity rather than useful data. The insula's uncomfortable signals of dread, aversion, or intuition are overruled by a learned mandate to stay uplifted, surrendered, faithful, or certain. In many cases this is a compensatory correction against a prior state of bitterness, suspicion, or collapse into distrust: the nervous system reaches for idealization because unbuffered cynicism feels intolerable. In relationship variants, it can appear as idealizing unavailable, exploitative, or grandiose partners, dismissing red flags as tests of love or faith, and repeatedly converting manipulation into a redemption story. In spiritual or superstitious variants, coincidence gets over-read as destiny, authority gets confused with wisdom, and the need for cosmic safety can override evidence, boundaries, and independent judgment. What looks like positivity is often a nervous system that cannot yet tolerate grief, disillusionment, uncertainty, or the pain of seeing clearly.
Our technique restores contact with reality without collapsing the person into despair or cynicism. We help the nervous system tolerate ambiguity, loss, and contradiction so optimism no longer has to be inflated into denial. We recalibrate the ventromedial prefrontal cortex's need for redemptive certainty, strengthen the anterior cingulate's capacity to stay with disconfirming evidence, and restore the insula's role as a source of valid internal warning rather than something to override with affirmations, prophecy, or charm. This is not an attack on hope, meaning, spirituality, or genuine faith. It is the restoration of grounded hope that can face facts. You experience less compulsive idealization, reduced susceptibility to manipulators and grandiose personalities, greater ability to distinguish trust from fantasy and reverence from submission, clearer perception of red flags without collapsing into paranoia, and a nervous system that no longer mistakes denial for faith or wish-based thinking for wisdom.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Relationship Jealousy & Insecurity
This could be your breakthrough. Let's do this!
Your partner's fidelity or commitment feels perpetually in doubt and your nervous system treats their other relationships as threats to your survival. Attachment became security-focused through hypervigilance. Relationship jealousy and insecurity involve persistent fear of abandonment, excessive monitoring of partner's whereabouts/communication, intense distress at partner's interactions with others, and behavioral or cognitive attempts to prevent infidelity or abandonment. Jealousy and insecurity often damage the relationship itself through their destructive impact on trust and autonomy despite stemming from fear of relationship loss.
The neurobiological mechanism involves insecure attachment patterns where the amygdala became conditioned to perceive partner separation or attention to others as abandonment threat. The ventromedial prefrontal cortex fails to maintain secure attachment representations during separation, leaving the amygdala persistently threat-activated when partner is unavailable or interacting with others. The insular cortex becomes hyperactive in monitoring social signals from the partner, interpreting neutral behavior as infidelity evidence. The anterior cingulate cortex generates persistent rumination about partner betrayal or abandonment. This hijacks the attachment system where security requires constant reassurance rather than secure base confidence.
Our technique recalibrates attachment security and amygdala threat-perception of partner separation through targeted limbic intervention. We restore secure base confidence where partner autonomy can be tolerated without triggering abandonment anxiety. Your nervous system ceases treating partner's other relationships as personal threat. You experience secure attachment, reduced jealousy and monitoring, and restored relationship quality.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Codependency & Relational Enmeshment
This could be your breakthrough. Let's do this!
Your sense of self became fused with other people's emotional states and you learned that your worth depends on meeting others' needs. Boundaries dissolved in service of perceived safety. Codependency involves loss of self in relationships, excessive caretaking or emotional responsiveness to others, difficulty setting boundaries, and personal needs subordination to maintaining relationships. Individuals with codependency typically manage others' emotions, abandon their own interests and preferences, and experience persistent anxiety when unable to control their partner's emotional state or maintain relational harmony.
The neurobiological mechanism involves overactive mirror neuron systems where others' emotions become neurally mirrored in the self, creating emotional fusion rather than empathetic connection. The medial prefrontal cortex fails to maintain clear self-other boundaries and instead activates for both self and intimate other similarly. The anterior insula loses accurate interoceptive awareness of personal needs and emotions, replaced by hyper-focus on others' emotional states. The amygdala becomes conditioned to others' emotional distress as personal threat requiring immediate management. Abandonment anxiety or rejection sensitivity drives compulsive relational caregiving where maintaining connection takes priority over self-care. The attachment system became addictive rather than secure.
Our technique restores self-other boundaries and personal autonomy through targeted limbic and identity intervention. We recalibrate interoceptive awareness of personal needs and reduce amygdala's reactivity to others' emotional states. Your nervous system restores clear sense of self separate from others. You experience healthy interdependence with maintained self-integrity, ability to set boundaries, and reduced compulsive caregiving.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Betrayal Trauma - Infidelity & Relational Violation
This could be your breakthrough. Let's do this!
Your nervous system learned that the person you trusted absolutely has done the one thing that proves you cannot trust anyone, and that your safety in intimate connection is now fundamentally compromised. Betrayal Trauma from infidelity or relational violation is a form of complex trauma where someone experiences profound rupture of their foundational attachment relationship. Unlike external trauma (assault, accident), betrayal trauma comes from the person whose presence should mean safety. The betrayed partner often experiences PTSD-like symptoms (intrusive images of infidelity, hypervigilance to partner's location/communications, emotional flooding), attachment terror (fear of abandonment or that they'll be betrayed again), and a shattered sense of reality ("I didn't know who I was married to").
The neurobiological mechanism involves simultaneous activation of threat-circuits and attachment-circuits, creating a state of irresolvable conflict in the limbic system. The amygdala becomes hyperactive to any stimulus associated with the betrayal (the location of infidelity, the time of day, reminders of the affair person), generating acute threat-response. The ventromedial prefrontal cortex's encoded narrative of the partner transforms from "safe attachment figure" to "threat," creating a state where the person's most important relational resource has become associated with danger. The hippocampus encodes fragmented traumatic memories of discovery or confrontation. The anterior insula becomes hyperresponsive to bodily distress and generates unbearable feelings of shame ("I wasn't enough," "I should have known," "I failed to notice"). The nucleus accumbens becomes dopamine-depleted not just for pleasure but for the specific person and relationship that should be rewarding but has become traumatic. The dorsolateral prefrontal cortex struggles to integrate the contradiction ("I love this person AND they betrayed me").
Our technique helps the nervous system process the betrayal as past trauma rather than continuing threat, separates the person's betrayal from the client's self-worth, and carefully works within the couple's attachment system to rebuild trust if repair is the goal. We recalibrate the amygdala's hyper-association between the partner and threat. We help the ventromedial prefrontal cortex integrate new information about the partner and relationship rather than remaining locked in the binary of "safe" or "threat." We resolve the anterior insula's shame and self-blame narratives. We support the nucleus accumbens's rewiring so attachment to the partner can potentially feel safe again (if repair occurs) or the person can fully disengage if the relationship is ending. You experience resolution of trauma symptoms related to the betrayal event, capacity to process the violation without it consuming your identity, and either genuine repair of the relationship on a more honest foundation or the clarity and closure to move forward separately.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Rejection Sensitivity Dysphoria
This could be your breakthrough. Let's do this!
Your amygdala treats subtle signs of rejection as social death threats. It's time to recalibrate that alarm. Rejection sensitivity dysphoria (RSD) is characterized by excessive emotional pain in response to perceived rejection, criticism, or abandonment, leading to hypervigilance to social cues indicating potential rejection. Individuals with RSD experience intense shame, rage, or despair in response to minor slights, perceived criticism, or situations where they might be excluded or judged. This hypersensitivity creates avoidance of social situations, perfectionist over-preparation to prevent criticism, and patterns of relationship dissolution when perceived rejection triggers explosive emotional responses. RSD is extremely common in ADHD, anxiety, and trauma populations.
The neurobiological mechanism involves amygdala hyperactivity combined with neural pathways that encode rejection as existential threat rather than minor social event. The anterior insula—which processes social pain—becomes hyperresponsive to rejection cues. Individuals with RSD have heightened neural processing of rejection that literally registers as comparable to physical pain. The amygdala becomes primed to detect rejection signals at the threshold of perception, leading to misinterpretation of neutral actions as rejection. The prefrontal cortex loses regulatory capacity once rejection-threat is detected. The nervous system becomes trapped in a state of perpetual vigilance to social threat.
Our technique recalibrates the rejection-threat response by resetting the amygdala's sensitivity to social cues through targeted limbic intervention. We dissolve the existential threat-perception in response to rejection and restore accurate social interpretation. Emotional pain in response to minor slights recedes as the nervous system distinguishes between genuine abandonment and minor social friction. This isn't resilience building or reframing. It's recoding of how your nervous system encodes rejection as threat. You experience restored calm in social interactions and genuine resilience to the inevitable minor rejections of social life.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Stockholm Syndrome - Trauma & Bonding
This could be your breakthrough. Let's do this!
Your nervous system bonded with an abuser because isolation and intermittent reinforcement hijacked your attachment system. Trauma bonding created the emotional glue that prevents escape. Stockholm Syndrome and trauma bonding involve the paradoxical experience of feeling love, loyalty, or protective feelings toward an abuser or captor despite ongoing abuse, threat, or captivity. Individuals in trauma bonds continue seeking contact with abusers, defend abusers against outside intervention, experience intense anxiety when separated from abuser, and often struggle to leave despite consciously recognizing abuse. The bond feels involuntary and stronger than rational understanding of danger.
The neurobiological mechanism involves amygdala sensitization to the abuser as the primary source of both threat and relief. In high-stress environments with intermittent reinforcement (cycles of abuse followed by sporadic kindness), the nervous system learns that the abuser is simultaneously both threat and safety. The ventromedial prefrontal cortex becomes dysregulated in threat-assessment, failing to accurately encode the abuser as persistent danger. The oxytocin bonding system becomes hijacked, generating attachment-related activation in response to the abuser rather than protective distance. The dorsolateral prefrontal cortex loses capacity for objective threat-assessment under the emotional pull of trauma-bonding chemistry. The nervous system becomes neurochemically addicted to the relief-after-threat cycle.
Our technique recalibrates the amygdala's threat-assessment and dissolves the trauma-bonding attachment through targeted limbic intervention. We restore accurate danger perception and sever the false therapeutic bond. Your nervous system regains capacity to recognize abusive patterns and activate protective rather than bonding responses toward abusers. You experience freedom from trauma bond, restored capacity to leave dangerous situations, and healthy attachment to safe people.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Loneliness and Social Disconnection
This could be your breakthrough. Let's do this!
Your nervous system learned that being around others activated threat. So it chose isolation. But isolation compounds the threat perception. Loneliness is a state of perceived social disconnection and dissatisfaction with social relationships—crucially different from solitude, which is restorative. Individuals with chronic loneliness experience persistent feelings of not belonging, rejection by groups or individuals, difficulty forming or maintaining relationships, and a sense of being fundamentally misunderstood or unable to connect authentically. This is devastating to health: loneliness has mortality risk equivalent to smoking 15 cigarettes per day. Beyond its health consequences, chronic loneliness creates a vicious cycle where the nervous system's threat-related behaviors (withdrawal, hypervigilance, defensive posturing) further alienate others.
The neurobiological mechanism involves dysregulation of the social brain systems. The amygdala becomes hyperactive to social threat while the ventral vagal complex—which enables safe social engagement—becomes suppressed. Individuals with chronic loneliness show heightened activation to potential social threats and reduced capacity to experience social reward and connection. Anxiety in social contexts drives withdrawal behaviors, which then confirm the prediction that connection isn't safe. The brain enters a state of social threat hypervigilance while simultaneously craving connection—creating internal conflict that drives isolated coping. The nervous system becomes trapped in a state where presence with others feels dangerous despite desperate longing for connection.
Our technique recalibrates social threat perception and restores social reward capacity through targeted limbic recalibration. We dissolve the amygdala hijack in response to social presence and restore ventral vagal engagement. Your nervous system regains capacity for genuine connection and authentic presence with others. This isn't skills training or social forcing. It's recoding of how your nervous system detects threat in social contexts. You experience restored capacity for belonging, authentic connection, and the vital health and wellbeing that emerges from genuine relationship.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Maternal Wound - Maternal Attachment Trauma & Mother Complex
This could be your breakthrough. Let's do this!
Your core template for receiving love was written by your mother, and that template is still running your intimate relationships. The maternal attachment wound is the foundational neural architecture that shapes adult capacity for closeness, trust, and emotional safety. Maternal attachment wounds occur when a child's earliest caregiver (typically mother) is unavailable, rejecting, inconsistent, enmeshed, or abandoning during critical periods of emotional development. The child develops specific neural patterns: desperate seeking of maternal approval despite repeated rejection, expectation of abandonment in intimate relationships, difficulty feeling worthy of love, tendency to attract partners who recreate the maternal wound (unavailable, critical, controlling), or conversely, compulsive caretaking to earn love that feels unearned.
The neurobiological mechanism: maternal attachment patterns become hardwired in the infant's oxytocin bonding system and amygdala threat-detection circuitry during the first two years of life when the mother is literally the child's entire world. If the mother is rejecting/withholding, the developing infant's ventromedial prefrontal cortex (responsible for self-worth and social safety) fails to develop healthy activation. The amygdala becomes hypersensitive to perceived rejection—a single withdrawn glance from the mother feels like existential threat and becomes encoded as persistent interpersonal danger. The oxytocin bonding system becomes dysregulated: bonding feels terrifying because the primary object of bonding was also the source of pain. Adult relationships unconsciously desperately seek a partner who will complete the unfinished maternal attunement, but the nervous system remains hypervigilant to maternal patterns of withdrawal, criticism, or control. Fear of abandonment drives either desperate pursuit or defensive emotional shutdown.
Our technique targets the maternal wound's neurological foundation by recalibrating the amygdala's threat-coding of maternal/feminine presence and restoring healthy activation of self-worth circuits. We identify the specific maternal patterns (rejection, enmeshment, control, emotional unavailability) and their neurological fingerprint in your threat-detection and bonding systems. Through creative reprogramming, we dissolve the desperate seeking of maternal approval and replace it with intrinsic self-worth. Your amygdala ceases hypervigilance to abandonment cues. Your oxytocin bonding system regains capacity to bond safely without recreating maternal trauma. Adult relationships transform from recreations of maternal wound to genuine partnership based on healthy choice rather than unfinished business.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Paternal Wound - Paternal Attachment Trauma & Father Complex
This could be your breakthrough. Let's do this!
Your father's presence or absence became your template for trust, safety, and whether the world is fundamentally secure. The paternal attachment wound shapes your capacity to access protection, guidance, and authentic masculine presence. Paternal attachment wounds occur when a child's father figure is emotionally unavailable, critical, abusive, absent (physically or emotionally), inconsistent, or fails to provide protection and safe-haven presence. In male children, paternal wounds create deep identity confusion about masculinity, difficulty accessing authentic strength and protection capacity, tendency toward either hyper-aggressive compensation or passive helplessness, or difficulty trusting male authority or male peers. In female children, paternal wounds create deep confusion about what safety with men feels like, desperate attraction to emotionally unavailable or dangerous males to "prove" one's worthiness of paternal love, difficulty believing men can be genuinely protective, or fear of male presence and authority.
The neurobiological mechanism: the father becomes the child's template for external safety and worldly protection—the one who provides safe-haven when the world feels dangerous. When the father is absent, abusive, or emotionally cold, the developing child's ventromedial prefrontal cortex (which encodes safety and protection) fails to develop healthy activation. The amygdala becomes hypersensitive to male presence and male authority as potential sources of harm. For males, the orbitofrontal cortex fails to develop healthy modeling of authentic masculine strength, so the nervous system either becomes hyper-aggressive (over-compensation) or helplessly passive. For females, the amygdala learns that male approvals feel life-threateningly important, creating either desperate attraction to unavailable males or fear of male power. The ventromedial prefrontal cortex encodes males as fundamentally untrustworthy. Adult romantic relationships become attempts to heal the paternal wound: females unconsciously seeking emotionally unavailable males hoping to "fix" the father, males seeking validation from partners because paternal approval was never internalized.
Our technique targets the paternal wound's neurological foundation by recalibrating the amygdala's threat-coding of paternal/masculine presence and restoring healthy activation of safety and protection circuits. We identify the specific paternal patterns (absence, abuse, coldness, inconsistency, failure to protect) and their neurological fingerprint in your threat-detection and trust systems. Through creative reprogramming, we dissolve the desperate need for paternal approval and the internalized belief that the world (or men) are fundamentally unsafe. Your amygdala ceases hypervigilance to male authority and male presence. Your ventromedial prefrontal cortex recodes men as potentially trustworthy and reliably protective. Adult relationships transform from desperate attempts to fix the paternal wound to genuine choice-based partnerships with men/people who offer genuine security and mutual respect.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Rescuer Syndrome - Caretaker Compulsion & Loss of Boundaries
This could be your breakthrough. Let's do this!
Your nervous system learned that your value comes from fixing, managing, and caring for others, and that your survival depends on making sure other people are okay. Rescuer Syndrome (the Rescuer role in Karpman's Drama Triangle) is a pattern where the person becomes compulsively focused on helping, supporting, fixing, and caretaking others to the point that their own needs are chronically unmet. The rescuer feels validated when needed and becomes anxious when others don't need their help. They often attract people in crisis (the "victim" role), creating cycles where the rescuer enables dysfunction while feeling righteous about their helping. The rescuer's relationships are characterized by severe boundary-collapse, difficulty saying no, resentment about imbalanced giving, and a profound loss of sense of self apart from caretaking.
The neurobiological mechanism involves dysregulation of empathy-and-helping circuits combined with profound attachment-wound and identity-fusion with caretaker role. The ventromedial prefrontal cortex encodes the belief "My worth comes from helping others" and "I only matter when I'm needed." The nucleus accumbens becomes dopamine-dependent on being needed, creating addiction to helping-behavior. The anterior insula becomes hyperresponsive to others' distress, making other people's suffering feel intolerable and driving compulsive helping attempts. The dorsolateral prefrontal cortex struggles with boundary-setting because boundaries feel selfish or cruel. The brain's "theory of mind" system becomes over-activated around others' needs and under-activated around personal needs. Early relational patterns (parentified child, emotionally responsible for parent) created these neural wiring patterns. The rescuer often experienced caregiving demands in childhood and learned that emotional acceptance and love were conditional on being helpful.
Our technique recalibrates the nucleus accumbens's helplessness-compulsion and helps the person find dopamine-reward in balance and self-care rather than in rescue-cycles. We reprogram the ventromedial prefrontal cortex's identity from "helper" to "whole person with value independent of usefulness." We modulate the anterior insula's hyper-responsiveness to others' distress so the person can be empathic without being compelled to fix. We activate the dorsolateral prefrontal cortex's capacity for healthy boundaries and help the word "no" feel safe and ethical. We address the early attachment wound that made worthiness conditional on caretaking. You experience freedom from compulsive helping, recovery of your own needs and desires, capacity for reciprocal relationships where both people give and receive, relief from resentment-cycles, and restoration of identity beyond caretaker role.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Financial Infidelity - Hidden Financial Transactions, Debt & Secret Money
This could be your breakthrough. Let's do this!
Your nervous system learned that hiding financial truth from your partner ensures your autonomy and safety, or that your partner cannot be trusted with honesty about money, or that your financial inadequacy is so shameful it must be concealed at all costs. Financial infidelity involves hiding financial transactions, debt, income, accounts, or financial decisions from a partner—a form of relational deception and betrayal that strikes at the foundation of relationship trust and partnership. The person may hide credit card balances, secret accounts, spending, debt, inheritances, or significant financial decisions from their partner, creating a parallel financial life that contradicts the illusion of transparency in the relationship. Financial infidelity is one of the leading causes of relationship breakdown and divorce, often causing more relational damage than sexual infidelity because it represents systematic betrayal and breach of fundamental partnership trust. The hidden financial life may be rooted in deep shame (inadequacy, inability to provide, history of financial failure), a need for control (assertion of autonomy through financial secrecy, fear of partner control), survival-protection (history of financial abandonment creating the need to maintain independent hidden resources), or adaptation to a controlling partner. During discovery, the partner experiences profound breach of trust, feelings of betrayal, loss of relational safety, and the realization that the financial partnership was built on lies.
The neurobiological mechanism involves dissociation between the person's behavior (hiding money) and their explicit values (commitment to partnership honesty). The ventromedial prefrontal cortex encodes financial information as "dangerous if known" based on early experiences (controlling parents, financial punishment, partner's past financial control or shaming). The amygdala becomes hyperactive to the prospect of financial transparency—vulnerability around money is encoded as mortal threat. The anterior cingulate cortex shows reduced impulse-inhibition and error-detection around financial deception—the person knows the deception violates partnership values but cannot override the amygdala's threat-response to transparency. The nucleus accumbens becomes dopamine-dependent on the relief-surge that comes from maintaining the secret and avoiding the threat of exposure. The medial prefrontal cortex develops bifurcated self-representation—one identity for the "honest partner" and one for the person who maintains financial secrets, creating compartmentalization. Often, profound shame about financial inadequacy, early experiences of financial betrayal, controlling parents or partners, or learned survival-patterns (hoarding hidden resources for escape) drive the deception. The person may experience genuine shame when discovered, or may feel suddenly seen and relieved, depending on whether the secret-keeping or the secrecy-necessity was the primary organizer.
Our technique first addresses the core threat-associations that made financial transparency feel dangerous: shame about financial standing, fear of partner control or judgment, early betrayal or abandonment trauma, or learned survival patterns of financial-autonomy-through-secrecy. We reprogram the ventromedial prefrontal cortex so financial transparency is encoded as safety and connection rather than as danger. We recalibrate the amygdala's threat-response to financial vulnerability and partner-knowledge. We restore the anterior cingulate's capacity for impulse inhibition and values-alignment. We dissolve the dopamine-reward from secret-keeping and help the nucleus accumbens discover greater reward-response to genuine transparency and partnership integrity. We integrate the bifurcated self-representations so the person can be genuinely congruent. We address any early trauma that established the deception-is-safety pattern and reprogram those pathways. We help the couples' mirror-neuron system and mentalizing capacity rebuild genuine empathy for the partner's experience of betrayal. You experience elimination of the anxiety-burden of secret-keeping, restored capacity for financial transparency without threat-response, genuine partnership integrity and relational embodiment of honesty, elimination of the compartmentalization and dissociation, rebuilt trust and safety within the partnership relationship, and financial systems organized around genuine partnership collaboration rather than hidden parallel systems.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Sexual Health & Dysfunction
Porn Addiction and Compulsive Sexual Behaviors
This could be your breakthrough. Let's do this!
Your nervous system became wired for a supernormal stimulus that surpasses natural sexual engagement in reward intensity. It's time to restore natural sexual motivation. Porn addiction and compulsive sexual behaviors are characterized by compulsive engagement in explicit sexual content or sexual activities despite negative consequences, loss of control, escalation (requiring increasingly extreme content), and functional impairment in relationships and other life domains. Individuals with sexual compulsivity experience erectile dysfunction or anorgasmia with partners due to overstimulation from extreme content, damaged intimate relationships due to deception or partner distress, sexual shame, and profound difficulty disengaging from compulsive patterns. This often co-occurs with loneliness and social anxiety.
The neurobiological mechanism involves hijacking of the sexual reward system by pornographic content engineered to maximize novelty and intensity beyond what natural sexual interaction can provide. The mesolimbic dopamine pathway becomes sensitized to porn-specific stimuli while showing tolerance to normal sexual stimuli, creating the sexually paradoxical situation where individuals feel strongly motivated toward porn but unable to become aroused by intimate partners. Anxiety and emotional avoidance drive compulsive use as a form of self-medication. The prefrontal cortex loses regulatory capacity as impulse control becomes increasingly insufficient. Shame and secrecy create additional anxiety loops that perpetuate compulsion.
Our technique recalibrates the sexual reward system and dissolves shame-based reinforcement loops through targeted limbic intervention. We restore prefrontal regulation and sexual motivation toward genuine partners. Compulsive porn use transforms into balanced sexual expression in relationships. This isn't abstinence advocacy or willpower training. It's recoding of how your nervous system encodes sexual motivation and processes intimacy-related anxiety. You access restored sexual responsiveness to partners and genuine capacity for intimate connection.
Related condition: Porn addiction and compulsive sexual behavior are distinct from Sex Addiction, though all three share dopamine dysregulation at the core.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Sex Addiction
This could be your breakthrough. Let's do this!
Your nervous system learned that sexual behavior is the primary mechanism for managing impossible internal states. Compulsive sexuality became your escape system. Sex addiction involves compulsive sexual behavior, masturbation compulsion, seeking multiple partners, risky sexual behavior, or sexual preoccupation that continues despite negative consequences including relationship damage, occupational impairment, risk of disease transmission, legal problems, and profound shame. Individuals with sex addiction experience loss of control over sexual behavior, escalation of sexual activity to achieve the same neurochemical effect, and temporary relief from anxiety or depression through sexual engagement before guilt and shame drive compulsion again.
The neurobiological mechanism involves dysregulation of the mesolimbic dopamine pathway where sexual behavior triggers supernormal dopamine release that exceeds natural sexual pleasure. The prefrontal cortex loses regulatory capacity, unable to inhibit sexual urges despite intellectual awareness of negative consequences. The amygdala becomes sensitized to emotional distress, anxiety, boredom, or loneliness as triggers for sexual behavior-seeking. The ventromedial prefrontal cortex fails to accurately weighing short-term sexual reward against long-term relationship and health consequences. Sexual behavior becomes the neurochemical solution to psychological distress, creating a self-perpetuating cycle where sexual relief is temporary, shame-rebound distress escalates need for more sexual engagement, and compulsion intensifies. Intimacy becomes secondary to sexual compulsion.
Our technique recalibrates the dopamine reward system and restores executive inhibition through targeted limbic intervention. We dissolve the distress-sexual-behavior link and restore genuine capacity for intimate sexuality. Your nervous system ceases using sexual compulsion as primary distress-regulation and accesses genuine emotional management alternatives. You experience freedom from sexual compulsion, restored capacity for authentic intimate sexuality with genuine partners, and integrated sexual expression.
Related condition: Sex addiction involves compulsive sexual behavior used for distress-regulation, distinct from Porn Addiction and Sexual Compulsivity though both involve dopamine dysregulation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Sexual Dysfunction - Impotence and Performance Anxiety
This could be your breakthrough. Let's do this!
Your nervous system learned that sexual performance is high-stakes threat assessment. It's time to restore authentic sexual presence. Sexual dysfunction encompasses erectile dysfunction (ED), premature ejaculation, anorgasmia, low libido and other sexual performance difficulties that significantly impact intimate relationships and self-esteem. Individuals with sexual dysfunction experience anxiety about sexual performance, shame about their bodies or abilities, avoidance of intimacy, and relationship conflict. Performance anxiety creates a vicious cycle where worry about dysfunction triggers the very physiological responses that prevent function.
The neurobiological mechanism involves performance anxiety hijacking the sympathetic nervous system (fight-or-flight) when parasympathetic activation is essential for sexual arousal and function. The amygdala perceives sexual performance as social threat to status and attractiveness, triggering anxiety that suppresses the parasympathetic tone necessary for sexual response. The prefrontal cortex becomes dominated by catastrophic performance predictions ('I'll fail again'), creating a self-fulfilling prophecy where anxiety prevents the relaxed state required for sexual function. Additionally, low dopamine from depression or stress reduces sexual motivation. The nervous system becomes trapped in a state where sexuality triggers threat-response.
Our technique recalibrates the amygdala's threat perception around sexual performance and restores parasympathetic activation through targeted limbic intervention. We dissolve the performance anxiety and restore authentic sexual presence. Erectile function, arousal capacity, and sexual motivation return as threat-detection resets. This isn't sexual technique training or gradual desensitization. It's recoding of how your nervous system processes sexual situations. You access genuine sexual confidence, restored function, and authentic intimate connection.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Anorgasmia - Orgasmic Disorder, Delay and Inability to Reach Sexual Release
This could be your breakthrough. Let's do this!
Your nervous system may be allowing sexual activation but refusing the final surrender into climax. Anorgasmia is a persistent or recurrent delay in, marked difficulty with, or absence of orgasm despite adequate desire, stimulation, and effort. It may be lifelong or acquired, generalized or situational, and often creates shame, frustration, relationship strain, and self-monitoring that further interferes with sexual responsiveness.
The neurobiological mechanism involves excessive cortical control, performance monitoring, sympathetic threat activation, and inhibition of the parasympathetic surrender required for orgasmic release. The amygdala may interpret full sexual expression as exposure, danger, or loss of control, while the insula becomes hyperaware of whether orgasm is happening quickly enough. The person begins tracking performance instead of inhabiting sensation, and orgasm becomes a pressure goal rather than an allowed reflex.
Our technique targets the threat and monitoring circuitry that block orgasmic completion. This is not a replacement for medical review, hormonal assessment, medication review, pelvic health care, or sexual technique education where those are needed. It addresses the fear-based overcontrol that prevents the nervous system from allowing full release. You experience greater embodied presence, less self-surveillance, and restored capacity to reach climax without the body or mind reflexively hitting the brakes.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Persistent Genital Arousal Disorder (PGAD) - Intrusive Unwanted Arousal & Pelvic Distress
This could be your breakthrough. Let's do this!
Your body may be generating sexual arousal signals that you did not choose and do not want. Persistent Genital Arousal Disorder (PGAD) involves recurrent or continuous genital arousal sensations, pressure, tingling, throbbing, or near-orgasmic urgency occurring without corresponding sexual desire. The condition is often profoundly distressing because the body appears sexually activated while the person feels invaded, frightened, exhausted, or desperate for the sensations to stop.
The neurobiological mechanism can involve dysregulated peripheral nerve signaling, pelvic floor overactivation, vascular factors, and central salience amplification by the brain. Once the sensations begin, the amygdala and insula often classify them as threatening, humiliating, or inescapable, which increases muscular guarding and attentional fixation. The person becomes trapped in a vicious loop where unwanted arousal causes panic, panic increases nervous-system gain, and the genital signal becomes even more intrusive.
Our technique targets the threat-amplification and pelvic vigilance loop that makes PGAD even more unbearable. This is not a replacement for pelvic neurology, gynecology, urology, medication review, or vascular assessment where needed. It addresses the nervous-system escalation that converts an already difficult sensory condition into a constant emergency. You experience reduced panic around the sensations, softer salience and body-monitoring, and a nervous system less likely to intensify the unwanted signal through fear.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Hypoactive Sexual Desire Disorder (HSDD) - Low Libido, Desire Loss & Intimacy Flatlining
This could be your breakthrough. Let's do this!
Your nervous system may have stopped treating sexuality as rewarding, safe, or relevant. Hypoactive Sexual Desire Disorder (HSDD) involves persistent lack of sexual desire, fantasies, or interest in sexual activity that causes distress. It often appears in long-term relationships as sexual desire discrepancy, where the absence of drive creates confusion, rejection, resentment, or fear that love itself has disappeared. The issue is not moral failure. It is a loss of motivational access to erotic engagement.
The neurobiological mechanism often involves dopamine depletion, stress chemistry, autonomic overactivation, shame encoding, relationship threat, or endocrine contributors that suppress the reward value of sexuality. The nucleus accumbens stops responding to erotic connection as strongly as it should, while the amygdala and prefrontal monitoring systems classify intimacy as pressure, duty, vulnerability, or performance risk. The person becomes detached from desire not because they are cold, but because the nervous system no longer marks sexual engagement as safe or rewarding.
Our technique targets the low-reward and high-threat coding that shut down desire. This is not a substitute for hormonal assessment, medication review, relationship therapy, or sexual medicine. It addresses the limbic and motivational circuitry that makes intimacy feel flat, pressured, or neurologically unavailable. You experience renewed access to desire, less dread around sexual engagement, and a nervous system that can once again register erotic connection as alive, safe, and worth moving toward.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Vaginismus - Pelvic Floor Guarding, Penetration Fear & Involuntary Spasm
This could be your breakthrough. Let's do this!
Your pelvic floor may be acting like a defense perimeter. Vaginismus involves involuntary tightening of the pelvic floor and vaginal entrance in anticipation of penetration or intimate contact, often making sex, tampon use, gynecologic exams, or even the thought of penetration painful, impossible, or deeply distressing. The condition is not a failure of desire or character. It is a real protective reflex encoded into the body, often intensified by shame, prior pain, fear, trauma, or repeated anticipatory dread.
The neurobiological mechanism involves threat-signaling through the amygdala, insula, autonomic nervous system, and pelvic floor motor circuitry. Sexual context becomes encoded as danger, causing protective bracing before conscious choice can intervene. The body begins guarding against pain, exposure, judgment, or loss of control. Once pain or failed attempts occur, the nervous system stores those experiences as confirmation that penetration is dangerous, making the next attempt even more reflexively defended.
Our technique targets the fear-bracing circuitry and helps the nervous system reinterpret intimate contact as safe rather than invasive. This is not a replacement for pelvic floor therapy, gynecologic care, trauma-informed sexual counseling, or medical evaluation where needed. It is targeted recalibration of the threat response that keeps the body clamping into protection. You experience reduced anticipatory fear, softer involuntary guarding, and restored capacity for consent-based intimacy without the body reflexively overriding you.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Fear of Intimacy and Commitment
This could be your breakthrough. Let's do this!
Your nervous system treats genuine closeness as existential threat. It's time to restore the capacity for authentic connection. Fear of intimacy is characterized by avoidance of emotional closeness, difficulty with vulnerability and self-disclosure, retreat when relationships deepen, and pervasive discomfort with being fully known by another person. Individuals with fear of intimacy often experience a paradox: they desperately want connection yet feel compelled to create distance or sabotage relationships as they become deeper. This creates a cycling pattern of brief attractions followed by withdrawal, leaving both individuals and partners confused and damaged.
The neurobiological mechanism involves an amygdala that learned through early attachment experiences that closeness is dangerous. When relationships deepen and vulnerability is required, the amygdala interprets this as existential threat to autonomy or safety. The nervous system activates protective disconnection—emotional numbing, critical thoughts about the partner, sudden loss of attraction, or creation of conflict. The ventral vagal complex, which enables safe social engagement, becomes suppressed when true intimacy is approached. The individual remains neurologically trapped in a state where genuine closeness triggers threat response.
Our technique recalibrates the intimacy-threat association by restoring secure attachment capacity and ventral vagal tone through targeted limbic intervention. We dissolve the false threat perception around vulnerability and authentic connection. Your nervous system regains capacity for genuine intimacy, authentic vulnerability, and sustained commitment. This isn't therapy process or gradual exposure. It's recoding of the neural patterns that learned to fear closeness. You access restored capacity for genuine intimate partnership and authentic connection.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Sexual Dysfunction & Intimacy Avoidance - Embodied Relational Healing
This could be your breakthrough. Let's do this!
Your nervous system learned through trauma, shame, or relational patterns that sexual intimacy is dangerous, shameful, or impossible, and your body has learned to shut down in response to sexual situations. Sexual Dysfunction and Intimacy Avoidance encompasses a range of conditions: difficulty with desire, arousal, or orgasm in sexual situations; pain with intercourse; erectile dysfunction; compulsive sexual behavior that lacks genuine intimacy; or avoidance of sexual contact altogether. These symptoms can stem from sexual trauma, relational conflict, performance anxiety, shame about bodies or sexuality, hormonal factors, or learned patterns of disconnection in intimate situations.
The neurobiological mechanism involves dysregulation of the parasympathetic "rest and digest" system required for sexual responsiveness combined with persistent sympathetic activation, amygdala hyperactivity around sexual situations, and prefrontal shutdown during arousal. The insula becomes hyperactive around bodily sensations, making physical intimacy feel threatening or distressing. The ventromedial prefrontal cortex encodes beliefs about sexuality as shameful, dangerous, or unwanted. The amygdala triggers threat-response to sexual touch or situations if there is trauma history. The nucleus accumbens becomes dopamine-depleted specifically around sexual reward if the person has experienced coercion or if sexual connection has become performance-based rather than pleasure-based. For trauma survivors, the body has learned that sexual situations are threat-contexts requiring shutdown or dissociation. The dorsolateral prefrontal cortex often becomes hyperactive (performance anxiety, monitoring self) in ways that prevent the prefrontal-quieting required for genuine intimacy.
Our technique helps the nervous system recognize safety in sexual situations by recalibrating threat-detection and activating the parasympathetic pathways required for genuine arousal and pleasure. We help the person reconnect with embodied sensation in gradually-paced ways that rebuild safety. We address trauma-related associations if present. We unwind performance-anxiety and self-monitoring that prevents genuine connection. We help couples rebuild genuine intimacy that isn't based on performance or obligation. We address shame-narratives about sexuality and the body. You experience reclaimed capacity for sexual pleasure and function, genuine intimate connection with your partner, freedom from sexual shame or performance anxiety, embodied presence in sexual situations, and sustainable sexual satisfaction.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Family, Parenting, Grief & Aging
General Attachment Issues
This could be your breakthrough. Let's do this!
Your earliest relationships wired your nervous system to expect particular relational patterns that now limit your capacity for secure connection. Attachment become the template for all relationships. General attachment issues encompass diverse insecure attachment patterns that developed from early relational experiences and now create dysfunction in adult relationships. Whether avoidant, ambivalent, fearful, or disorganized patterns, insecure attachment creates persistent relationship difficulties, emotional distance, pursuit-withdrawal cycles, or paradoxical distance-seeking in intimate relationships.
The neurobiological mechanism involves the ventromedial prefrontal cortex encoding relational expectations and secure base representations based on early attachment experiences. When early caregivers were inconsistently available, rejecting, or overwhelming, the amygdala became hyperactive to abandonment or engulfment threat during adult closeness. The mirror neuron systems may become dysregulated, affecting capacity for emotional resonance and empathetic attunement. Insecure attachment patterns activate in adult relationships, triggering protective responses (distancing, pursuing, shutting down) that recreate the early relational pattern. The attachment system uses these patterns as safety strategies despite their actual relationship-damaging effects.
Our technique recalibrates the attachment security representations through targeted limbic and relational intervention. We dissolve the early attachment trauma pattern and restore capacity for secure adult attachment. Your nervous system regains capacity for genuine closeness with maintained autonomy and healthy dependence. You experience secure attachment patterns and restored capacity for fulfilling intimate relationships.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Abandonment Trauma & Hyper-Vigilance - Teen Rejection Sensitivity
This could be your breakthrough. Let's do this!
Your adolescent is desperately scanning for signs of rejection, reading minute social cues as abandonment-signals, and living in constant fear that the people they care about will leave. Adolescent abandonment trauma and hyper-vigilance occur when a teen has experienced parental abandonment, parental death, family dissolution, or earlier childhood neglect, and the adolescent's nervous system remains locked in abandonment-detection mode. The amygdala becomes hypersensitive to any sign of rejection or disconnection: a parent's delayed text becomes evidence of abandonment, a friend's busy schedule becomes evidence of not-caring, peer group changes become evidence of being rejected. The adolescent may engage in desperate clinging behaviors, people-pleasing to maintain relationships, compulsive reassurance-seeking, or conversely, preemptive relationship-abandonment ("I'll leave before they leave me"). The adolescent's entire social strategy becomes organized around abandonment-prevention.
The neurobiological mechanism: the amygdala has been conditioned (by actual abandonment experience) to code disconnection-signals as fundamental threat. The oxytocin bonding system has been damaged—bonding feels unsafe because the primary object of bonding abandoned. The ventromedial prefrontal cortex encodes relationships as fundamentally unsafe/unstable. The insula becomes hyperresponsive to social exclusion cues. The nucleus accumbens becomes dopamine-sensitized to reassurance and reconnection, driving desperate reassurance-seeking. The anterior cingulate cortex is in constant conflict-monitoring as the adolescent reads every social interaction for abandonment-evidence. The medial prefrontal cortex encodes the self as unworthy of stable connection ("If I mattered, they wouldn't have left").
Our technique addresses the actual abandonment trauma and helps the amygdala recalibrate abandonment-threat-assessment. The ventromedial prefrontal cortex rebuilds safety-template for relationships. We help the adolescent distinguish between actual rejection-signals and amygdala over-interpretation. The oxytocin system has opportunity to rebuild secure bonding with consistent, reliable adults. The nucleus accumbens decouples from reassurance-seeking dopamine and finds reward in genuine connection instead. The adolescent develops secure attachment capacity, decreased abandonment-panic, ability to tolerate normal disconnection without existential threat, and healthier relationship dynamics not driven by abandonment-terror.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Divorce? - Relational Trauma and Family Systems Stress
This could be your breakthrough. Let's do this!
Relationships don't fail because love dies. They fail because the nervous systems learned to perceive each other as threat. Relational trauma and family systems stress represent a unique category of psychological injury that occurs within intimate relationships and family units where there is chronic conflict, invalidation, or breakdown of the attachment bond. Whether triggered by ongoing marital discord, divorce proceedings, or long-term family instability, these experiences create continuous psychological threat that pervades daily life.
The mechanism of relational trauma operates through a feedback loop of collective limbic hyper-vigilance where neutral interactions become perceived as threats to safety and belonging. Chronic anxiety within marriage or family units creates elevated baseline tension where each family member becomes hypersensitive to potential criticism or rejection. When conflict escalates, this triggers 'flooding,' a physiological overwhelm that shuts down the prefrontal cortex and prevents the empathy and logical processing required for conflict resolution or healing dialogue.
Our technique works with the nervous systems of both partners to recode the threat-detection loop that perpetuates conflict. Through creative reprogramming of limbic patterns, we interrupt the automatic reactivity and replace it with genuine empathy, understanding, and collaborative capacity. This is not couples therapy or communication training. It is precision recalibration of how your nervous system responds to your partner's presence and vulnerability. Relationships transform from conflict-locked loops to genuine connection and safety.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Adult Children of Alcoholics - Intergenerational Trauma Pattern
This could be your breakthrough. Let's do this!
Your nervous system learned early that one parent's addiction meant you could never truly rely on consistent care, and that you had to become hyper-responsible to manage the chaos and dysfunction. Adult Children of Alcoholics (ACA) describes individuals who grew up in homes where at least one parent had an active or unmanaged addiction, and who experienced the chronic psychological consequences: unpredictability, emotional neglect despite physical presence, parentification (having to parent the parent or siblings), fear of the addicted parent when intoxicated, and the deep internalized belief that your needs were secondary to the addiction.
The neurobiological mechanism involves early dysregulation of the attachment system combined with hyperactivated stress-response and disrupted sense of self-worth. The insecure attachment styles developed in response to an unreliable caregiver persist into adulthood, creating fear of abandonment and difficulty trusting others' constancy. The amygdala becomes hypervigilant to signs of unpredictability, loss of control, or threats to safety—patterns directly learned from living with addiction's chaos. The ventromedial prefrontal cortex encodes profound beliefs about inadequacy ("If my love was enough, they wouldn't drink") and danger ("Relationships are unpredictable and potentially explosive"). Parentification creates a dysregulated sense of responsibility where the person feels they should manage others' emotions and problems despite being powerless to do so. The hippocampus stores fragmented memories of frightening intoxication events or emotional chaos. ACAs often unconsciously recreate the dynamics of their origin family: selecting partners with addictive tendencies, over-functioning in relationships, struggling with boundary-setting, and experiencing shame about their family history.
Our technique recalibrates the amygdala's hypervigilance to unpredictability and helps the person distinguish between genuine danger and triggers from the past. We rebuild secure internal attachment by healing the early relationship wounds and developing capacity to trust reliability. We reprogram the ventromedial prefrontal cortex's beliefs about inadequacy and replace them with realistic understanding of what could and couldn't be controlled as a child. We reset the dysregulated responsibility-circuits so the person can distinguish between healthy responsibility and trauma-driven over-functioning. We help the person break the unconscious pattern of selecting partners who recreate the family dynamics. You experience freedom from compulsive caretaking and over-responsibility, capacity to build healthy relationships outside addiction-trauma patterns, genuine understanding of what was and wasn't your fault as a child, and interruption of the intergenerational trauma transmission.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Family Scapegoat & Identified Patient Pattern - Blame Displacement in Dysfunctional Systems
This could be your breakthrough. Let's do this!
Your family system may have organized its anxiety, shame, conflict, or instability around making one person carry what the whole system cannot face. The family scapegoat pattern occurs when one member becomes the designated problem, disappointment, rebel, sick one, difficult child, or "identified patient" whose symptoms or behavior are treated as the source of the family's distress. In reality, the scapegoated person is often expressing or absorbing tensions that belong to the entire system. This role can emerge in families marked by trauma, addiction, personality disturbance, rigid hierarchy, favoritism, emotional immaturity, or chronic denial. The scapegoated person often grows up confused, over-blamed, hypervigilant, and deeply split from their own sense of innocence and reality.
The neurobiological mechanism involves chronic attachment threat combined with group-level blame displacement. The family system uses projection to externalize intolerable shame, aggression, grief, or chaos onto one member, while that person's amygdala becomes conditioned to expect accusation, exclusion, and misinterpretation. The insula becomes hyperreactive to signs of disapproval, making even neutral interactions feel like imminent indictment. The ventromedial prefrontal cortex can internalize the role itself, encoding beliefs such as "I am the problem," "I ruin everything," or "I must either disappear or fight to exist." At the same time, other family members gain temporary relief and false cohesion by keeping distress localized in one person rather than confronting systemic dysfunction.
Our technique targets the nervous-system imprint of being made to carry collective blame. We help separate the person's authentic self from the role assigned by the family, reduce hypervigilance to accusation and exclusion, and restore reality-testing where the entire system's dysfunction is no longer encoded as personal defect. This is not about rehearsing resentment or proving one side morally pure. It is recalibration of the attachment-trauma and shame circuitry created by chronic blame displacement. You experience relief from the internalized belief that you are the family's problem, stronger self-trust, less automatic collapse in the face of criticism, and restored capacity to form relationships where you are not unconsciously cast as the container for everyone else's pain.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Parenting Stress, Anxiety & Inadequacy - Parental Overwhelm
This could be your breakthrough. Let's do this!
You are responsible for another human's survival, development, and wellbeing—and your nervous system knows it could fail at any moment. Parenting stress, anxiety, and feelings of inadequacy arise when a parent's nervous system becomes locked in a state of hypervigilance where the amygdala is constantly scanning for all the ways a child could be harmed, neglected, or disappointed. Parents experience intrusive thoughts ("What if I'm damaging the child?"), chronic tension and irritability, inability to enjoy parenting moments due to threat-scanning, perfectionism about parenting performance, comparison-driven shame ("Other parents do this better"), and difficulty believing they are "good enough" as a parent despite evidence to the contrary. The inability to soothe internally means external chaos from children triggers rapid nervous system dysregulation.
The neurobiological mechanism: parenting engages the anterior insula (social pain and responsibility-detection), the posterior cingulate cortex (self-related thinking and identity), and the amygdala (threat-detection for both the child's safety AND the parent's competence). When a parent's own childhood was chaotic, neglectful, or abusive, their nervous system learned that parenting = danger and shame. The prefrontal cortex fails to communicate safety-signals to the amygdala ("You are a capable parent"). The anterior insula becomes hyperactive to any sign of a child's distress—the nervous system interprets a child's crying as proof of parental failure. The brain becomes unable to distinguish between real danger and developmentally normal childhood challenges. Dopamine dysregulation means the parent cannot access the reward/pleasure of parenting—only the anxiety. The parent becomes locked in reactive parenting mode where everything feels urgent and catastrophic.
Our technique recalibrates the amygdala's threat-coding around parenting responsibility and restores the prefrontal cortex's capacity to evaluate realistic parenting adequacy. We dissolve the linkage between a child's normal distress and the parent's experience of personal failure. Your nervous system learns that you can be a good-enough parent without being perfect, that your child's emotions are separate from your worth, and that parenting challenges are normal, not proof of incompetence. The anterior insula recodes your child's needs as solvable problems rather than existential threats to your identity. You access the genuine joy and presence available in parenting, manage challenges with calm capability rather than reactive panic, and develop intrinsic confidence in your parental adequacy.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Co-Parenting & Custody Conflict - Family Separation Anxiety
This could be your breakthrough. Let's do this!
Your nervous system is caught in a family system torn apart by parental conflict, custody disputes, and separation distress. This affects both parents managing co-parenting disagreement and the non-custodial parent's separation anxiety from their child. Co-parenting conflict occurs when separated, divorced, or never-married parents have dramatically different parenting values, styles, or emotional capacity, and lack the capacity to subordinate their adult conflict to the child's developmental needs. Simultaneously, one or both parents may experience intense separation anxiety around custody transitions, fear of missing significant moments, and anxiety that the other parent is displacing their role in the child's life.
The experience is multi-layered: Children become caught in the middle of parental conflict, experiencing split loyalties, fear of expressing love for one parent (perceived as betrayal), and nervous system stress during custody exchanges as threat-events. Non-custodial parents experience intense separation distress during visitation departures, obsessive contact attempts, or defensive emotional withdrawal. Both parents' amygdalae become dysregulated from the presence of the co-parent, activating threat-detection circuits from the original relationship conflict. Each parent's insula becomes hyperactive to perceived threats to the child's wellbeing based on co-parent choices. Parents weaponize parenting decisions as proxy battles for the original relationship conflict. Children develop fragmented identities, unable to integrate across family systems. Non-custodial parents encode themselves as devalued ("You matter less because you have less time").
The neurobiological mechanism is complex: The amygdala becomes dysregulated in both parents from co-parent presence and from separation/visitation schedules acting as threat-events. Each parent's prefrontal cortex loses capacity to think rationally about the co-parent's intentions or evaluate decisions based on child's interests rather than malintent. The child's amygdala synchronizes with both parents' dysregulated states. The ventromedial prefrontal cortex fails to provide coherent "family" understanding or self-worth independent of parental conflict. Non-custodial parents' nucleus accumbens becomes dopamine-depleted during separation, creating withdrawal-like states. Parent's own childhood abandonment becomes reactivated with each visitation transition. Children's reward circuits become dysregulated—bonds feel conditional on loyalty to parenting ideology rather than secure and safe.
Our technique addresses both the co-parenting conflict dysfunction and the separation anxiety simultaneously. We recalibrate each parent's amygdala response to the co-parent, separating original relationship injury from current co-parenting function. We help parents understand that effective co-parenting is an adult responsibility—cordial functioning with someone you're no longer in love with, not reconciliation. We dissolve the linkage between the child's relationship with the co-parent and the parent's abandonment/betrayal/loss. We target the amygdala's false encoding of visitation transitions as actual abandonment, recalibrating neural representations of time ("separation has an endpoint") and safety ("relationship is continuous even apart"). Non-custodial parents' dopamine system learns to find reward in quality time rather than being depleted by absence. We create protocols for communication that disable threat-activation from original conflict. Children experience the nervous system relief of both parents committed to their wellbeing, consistent parenting values across homes, and freedom to love both parents without guilt. Parents experience capacity to be fully present during their time with the child, comfort with child's attachment in other home, and freedom from anxious monitoring that damages relationships.
Related condition: Children caught in this dynamic frequently develop Adolescent Abandonment Trauma & Hyper-Vigilance as they mature, internalizing both parental conflict and separation anxiety.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Step-Family & Blended Family Integration Stress - Family System Transition
This could be your breakthrough. Let's do this!
Blended families require an entire nervous system recalibration: new parental authorities to bond with or resist, sibling-like relationships with instant strangeness, territory and belonging boundaries that are undefined, loyalty conflicts (loving the step-parent feels like betrayal of the biological parent), and the grief of the original family structure. Step-family and blended family adjustment issues occur when children and adults lack a clear belonging-template for the new family system. Children experience confusion about who they belong to, what loyalty they owe, what rules apply and who enforces them, whether the step-parent is a replacement or an addition, and fear of losing the non-custodial parent if they bond with the step-parent. Adults experience conflict between biological and step-children, guilt about the impact of family restructuring, difficulty enforcing authority as a step-parent, and uncertainty about their role in the new family hierarchy.
The neurobiological mechanism: the amygdala becomes dysregulated by the presence of new authority figures and the disruption of established attachment patterns. The child's neural map of "family" becomes confused—the original parent's absence creates a threat-response (abandonment), while the new parental figure creates simultaneous feelings of replacement-threat. The insula becomes hyperactive to unfamiliar family members' presence and behaviors. The ventromedial prefrontal cortex fails to generalize trust from the original family structure to the blended family, so each new interaction feels unsafe. Children experience loyalty conflicts because the reward circuits (oxytocin bonding) become split between the biological and step-parents. The anterior cingulate cortex struggles with the cognitive dissonance of new family rules, new authority structures, and new intimacy expectations. The orbitofrontal cortex fails to develop a stable "family value system" because there appear to be competing value systems in the new family constellation.
Our technique stabilizes the amygdala's response to family restructuring by creating clear neural maps of belonging, role clarity, and revised family identity. We dissolve loyalty conflicts by helping each family member understand that bonding with a step-parent is addition, not replacement. The child's ventromedial prefrontal cortex learns that the blended family structure is safe and trustworthy despite being different. Each family member's role becomes clear in the nervous system—what authority each person holds, what intimacy each relationship involves, and how the new family creates coherent values. The amygdala recodes the step-sibling and step-parent presences as part of the safe family, not as intruders or threats. Family members experience reduced conflict, clearer communication, and the capacity to build genuine affection across blended family boundaries.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Foster Family Integration & Reactive Attachment - Adolescent Placement Disruption
This could be your breakthrough. Let's do this!
Your adolescent has learned that families are temporary, caregivers leave, and bonding leads to loss. Teen foster family integration and reactive attachment issues occur when an adolescent in foster care or other out-of-home placements has experienced multiple family losses and cannot trust that the current placement will be permanent. The reactive attachment involves: difficulty accepting care from new caregivers, testing behaviors designed to provoke rejection (confirming the belief that they're unlovable), inability to use the caregiver as a secure base, superficial charm mask combined with emotional distance, or aggressive resistance to belonging attempts. The adolescent's oxytocin bonding system has been damaged by repeated separation/loss. The amygdala codes new caregiver-attachment as dangerous (previous caregivers left). The ventromedial prefrontal cortex encodes the self as inherently unlovable. The prefrontal cortex generates testing behaviors ("I'll show them they're right to leave before they leave voluntarily").
The neurobiological mechanism: reactive attachment develops from repeated experience of inconsistent caregiving, neglect, or separation during critical bonding windows. The oxytocin system becomes dysregulated—bonding impulses are mixed with fear-of-abandonment. The amygdala maintains residual threat-response to caregiver-closeness (previous closeness = previous abandonment). The insula becomes hyperresponsive to signs of caregiver disconnection. The ventromedial prefrontal cortex has never encoded reliable caregiver-safety. The nucleus accumbens has not learned to find dopamine-reward in caregiver-connection. Testing behaviors are neurologically automatic—designed to activate the amygdala's anticipated abandonment.
Our technique helps foster families understand that testing-behaviors are not malice but nervous-system checking ("Is this caregiver going to leave? Let me test."). We provide psychoeducation about reactive attachment and skill-building for caregivers. We support the oxytocin system's slow rebuilding through consistency, safety, and non-rejection-response to testing. The amygdala gradually recodes consistent caregiver-presence as safe rather than dangerous. The ventromedial prefrontal cortex rebuilds relational safety-template. The adolescent gradually develops secure attachment capacity with the current placement and experiences decreased testing behaviors, restored capacity for genuine relationship, decreased fear of abandonment, and potential for genuine family integration and permanency.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Runaway Behavior & Elopement - Adolescent Escape Response
This could be your breakthrough. Let's do this!
Your adolescent's nervous system determined that being in the current environment (home, placement, family) is worse than the unknown danger of running away. Teen runaway behavior and elopement occur when an adolescent abandons their home or placement as the only solution to an unsustainable situation. Runaways are typically not impulsive—they represent a deliberate calculation that the dangers of the current environment exceed the dangers of the unknown. The teen may run due to family abuse/trauma, family rejection, placement disruption, peer crisis, feeling unwanted/not-belonging, or escape from consequences. Upon running, the teen faces genuine dangers (trafficking predators specifically target runaways, homelessness, starvation, violence, forced criminality). Many runaways have experienced previous abuse/trauma and have reasonable threat-assessment about family danger—they're not wrong to leave, but they leave without external safety-network and become vulnerable to worse danger.
The neurobiological mechanism: family/placement generates chronic fear or rejection-activation in the amygdala. The ventromedial prefrontal cortex encodes "being in this environment" as threatening to survival. Running away becomes the amygdala's solution—better unknown danger than known threat. The adolescent's future-planning systems (dorsolateral prefrontal cortex) are underdeveloped and fail to generate adequate risk-assessment of runaway dangers. The oxytocin bonding system with caregivers has been damaged (family abuse, rejection, or failed bonding attempts). The risk-reward processing of the nucleus accumbens is dysregulated and the short-term escape-dopamine outweighs long-term survival-risk. Traumatized teens' threat-assessment is often accurate (this family/placement IS unsafe)—but the running away solution escalates danger rather than solving it.
Our technique begins with meeting the adolescent's actual need (safety from the threat they're running from) rather than simply forcing return to the dangerous environment. If family is genuinely abusive/rejecting, real alternative safety is required. If placement is failing, effective re-placement is needed. We help the amygdala's threat-assessment become accurate about which environments are genuinely dangerous vs. which are merely containing/limiting. The ventromedial prefrontal cortex develops genuine problem-solving that doesn't require running. The oxytocin system has opportunity to potentially rebuild bonding with safer caregivers. The adolescent experiences genuine safety in the environment, restoration of family connections (if safe), or stable alternative placement, and decreasing need for escape-behavior because the current environment no longer feels survival-threatening.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Empty Nest Syndrome - Marital Disconnection & Identity Loss After Parenting Role Ends
This could be your breakthrough. Let's do this!
Your nervous system organized your identity and your marriage around the central role of parenting, and now that role is gone, you face a crisis of purpose, identity, and relational connection with your partner. Empty nest syndrome in the context of marriage is characterized by profound disorientation when children leave home—the individual experiences the loss of a primary life role, identity, and source of daily purpose. More critically for marriages, many couples realize that the shared project of parenting was the primary structural foundation holding the relationship together. Without the buffer of child-rearing responsibilities, the couple confronts the actual strength (or fragility) of their own romantic connection—often discovering they lack genuine intimacy, shared interests, or healthy communication patterns. The partner who was more invested in the parenting role often experiences a distinct identity collapse: "Who am I if I'm not actively parenting?" The marriage itself may come into crisis as both partners simultaneously experience this loss while having depleted emotional resources from two decades of child-focused caregiving. Common presentations include depression, anxiety, identity confusion, relationship conflict escalation, infidelity, rediscovery of addiction or escape behaviors, or parallel-living in which the couple remains together but emotionally disconnected.
The neurobiological mechanism involves the collapse of the default-mode network's narrative about life meaning and identity. The ventromedial prefrontal cortex (meaning-making and self-representation) has been organized for 18-25 years around the role of "parent" and the shared dyadic role of "co-parenting team"—when that role suddenly ends, the medial prefrontal cortex experiences a kind of identity deletion error, creating acute existential distress. The nucleus accumbens, which has been dopamine-responsive to parenting rewards (children's achievements, family stability, role fulfillment), suddenly receives no reward signals from those behaviors—depression and anhedonia result. The anterior cingulate cortex, which has been hyperactive in error-monitoring and conflict-resolution related to child-rearing, now extends this hyperactivity to the marital relationship itself, increasing perception of relationship errors and conflicts. The orbitofrontal cortex, which encoded the shared value-system of the couple as parents, now confronts a potential mismatch in deeper personal values—each partner may discover the other's actual interests, needs, and priorities now that parenting is not the organizing framework. The mirror neuron system and mentalizing circuits may show reduced activation between partners as they've spent years cooperating on child-rearing while avoiding intimate vulnerability. The amygdala becomes hyperresponsive to potential abandonment or relationship dissolution as the couple faces the real question: "Do we actually want to be together?" Often, one or both partners have spent 20 years in a parenting role that provided clear structure, validation, and meaning, and now face an existential void. The person's sense of worth has been fused with "good parent" identity, and losing that role creates profound shame and worthlessness feelings. The relationship may have been maintained by avoidance of intimacy through the constant demands of child-care—now there's nothing to avoid with, and the couple must address either genuine reconnection or the true dissolution of the marriage.
Our technique helps you rebuild identity independent of the parenting role while simultaneously rebuilding genuine intimacy with your partner. We help the medial prefrontal cortex develop a coherent post-parenting identity with intrinsic meaning beyond child-rearing. We restore dopamine responsiveness to authentic partnership, genuine conversation, shared experiences, and mutual vulnerability rather than to parenting role-fulfillment. We reduce the anterior cingulate's hyperactive conflict-scanning and help the couple develop genuine conflict-repair skills rather than parenting-focused cooperation. We help the orbitofrontal cortex re-discover or establish genuine shared values and interests independent of children. We restore mirror neuron resonance and mentalizing capacity between partners through practices of genuine emotional attunement and risk-taking vulnerability. We help each partner grieve the loss of the active parenting identity while building acceptance of genuine mid-life redirection. We address any infidelity, addiction, or escape-behavior reactivation as a symptom of the underlying identity and relationship crisis rather than as a character failure. If the partnership is genuinely incompatible, we help the couple consciously choose separation rather than years of resentful co-habitation. If the partnership has genuine foundation, we help rebuild authentic intimacy and discover new shared meaning in the second act of marriage. You experience integration of post-parenting identity with authentic self, genuine emotional and relational reconnection with your partner (or conscious healthy dissolution), restoration of meaning and purpose beyond parenting, and potential emergence of a mature, intimate partnership based on authentic choice rather than logistical necessity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Complicated Grief Disorder - Persistent Bereavement
This could be your breakthrough. Let's do this!
Your nervous system learned that the death of your loved one is an event that should not have happened, and that your survival depends on refusing to accept their absence. Complicated Grief Disorder (also called Persistent Complex Bereavement Disorder) is a condition where grief responses become stuck, preventing the natural progression toward acceptance and meaning-making. Rather than gradually integrating loss and moving forward, the person remains hyperactivated in acute grief, with intense yearning, strong resistance to the reality of death, and difficulty engaging with life without the deceased person. Months extend to years, and the person's world remains frozen around the moment of loss.
The neurobiological mechanism involves dysregulation of the default mode network (which handles self-referential thought and meaning-making) combined with amygdala hyperactivity and ventromedial prefrontal cortex failure to update threat appraisal. The amygdala continues to treat the loss as an ongoing threat requiring survival response rather than a past event to be integrated. The anterior cingulate cortex becomes locked in persistent expectation mismatch—the person knows cognitively that the deceased is gone but the limbic system keeps expecting their return, creating perpetual cognitive dissonance. The nucleus accumbens becomes dopamine-depleted not just for pleasure but for the specific reward-neural-pathways that connected to the deceased person—the person has lost not just the person but the entire neurochemical reward system built around them. The medial prefrontal cortex fails to generate the self-perception update required to integrate "I am someone living without them." The default mode network can't generate the meaning-narrative that would transform "I lost this person" into "I live carrying their memory" or "I honor their life by living fully."
Our technique recalibrates the amygdala to recognize loss as integrated past rather than ongoing threat. We help the anterior cingulate resolve the expectation mismatch by creating new neural pathways that accommodate absence as new reality. We rebuild the nucleus accumbens's capacity to find dopamine-reward in a life that no longer includes the person's daily presence. We reconstruct the medial prefrontal cortex's self-narrative to integrate loss while maintaining identity continuity. We help the default mode network generate meaning from grief that honors the relationship while releasing the person to continue living. You experience completion of the grief process rather than frozen perpetual bereavement, integration of loss into your life narrative rather than avoidance of reality, renewed capacity for joy and engagement without guilt, and transformation of the relationship from active presence to honored memory.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Identity Loss in Aging - Loss of Life Role & Purpose
This could be your breakthrough. Let's do this!
Your nervous system learned that your identity was your work, your productivity, your role as provider or caregiver or professional, and now that these roles have been removed by retirement or life circumstance, you don't know who you are anymore. Identity Loss in Aging is an existential and developmental challenge where older adults experience profound confusion about self when the roles and functions that defined them are no longer available. This may be triggered by retirement, loss of work identity, role as active parent (children grown), loss of physical abilities that defined self-concept, or transition to elder status in culture that devalues aging. The person may experience this as depression, meaninglessness, or directionlessness rather than recognizing it as identity-reconstruction challenge.
The neurobiological mechanism involves the medial prefrontal cortex's self-concept being architecture built primarily on role and function, leaving empty space when those external roles are removed. The ventromedial prefrontal cortex has encoded the person's value as conditional on productivity, creating crisis when productivity ends. The default mode network, which handles self-referential thinking, becomes hyperactive in rumination without the external structure of work/role to provide meaning-scaffolding. The anterior cingulate cortex struggles to integrate the new life phase while reflexively grasping toward the old one. The nucleus accumbens shows reduced stimulation from the environmental rewards that used to come from role-based engagement. The person often has never practiced self-definition separate from their function, leaving them neurologically under-equipped to answer "Who am I?" without external role-definition.
Our technique helps the medial and ventromedial prefrontal cortex rebuild identity that encompasses continuity from the old life while being constructed from new foundations. We help the default mode network transition from rumination and role-loss grief to exploration of authentic interests and values. We support the nucleus accumbens in discovering new sources of reward and engagement in this life phase. We help the person genuinely integrate aging as a positive life stage rather than experiencing it as diminishment. We facilitate the psychological work of elder self-definition that includes wisdom, relationships, legacy, personal growth, and contribution in new forms. You experience clarity about who you are beyond your former roles, renewed sense of purpose and meaning in this life chapter, engagement in activities that feel authentically valuable rather than role-based, and integration of aging as a positive developmental stage with its own richness.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Anticipatory Grief - Fear of Impending Loss
This could be your breakthrough. Let's do this!
Your nervous system is locked in existential rehearsal: practicing the death that has not yet occurred, unable to fully be present to the person who is still alive, terrified of the loss that is coming. Anticipatory Grief occurs when a person faces the imminent loss of a loved one who is terminally ill or declining (from illness, dementia, aging), and the neurological system becomes hyperactivated in pre-loss processing. The person oscillates between moments of connection with the living person and intense grief-processing about their future absence. They may find themselves emotionally saying goodbye while the person is still present, unable to balance presence with protection against future pain. The loss has neurologically already begun even though the death has not yet occurred.
The neurobiological mechanism involves premature activation of the grief-processing systems before the loss has actually occurred, creating a state of chronic threat-anticipation combined with ongoing relational connection. The anterior cingulate cortex becomes hyperactive in prediction about future loss, generating persistent low-grade anxiety about what is coming. The amygdala learns to treat the present moment as already threatening because of what's coming, preventing authentic presence. The insula generates persistent bodily distress about impending loss. The ventromedial prefrontal cortex becomes split between two incompatible realities: "This person is alive and here with me now" and "This person will no longer exist in my life soon." The nucleus accumbens becomes conflicted between the reward of present connection and the prediction of future dopamine-depletion from loss. The person may emotionally withdraw from the dying person as a protective strategy ("If I can't be close now, the loss will hurt less"), but this creates double loss: losing both the person's presence now and their relational engagement. Caregiving exhaustion often compounds anticipatory grief.
Our technique helps the nervous system hold two truths simultaneously: present connection and impending loss, without the present becoming consumed by fear of the future. We recalibrate the anterior cingulate's hyperactive loss-prediction so it becomes realistic planning rather than chronic threat-response. We help the insula modulate the bodily distress of anticipatory grief while maintaining somatic presence. We stabilize the ventromedial prefrontal cortex's capacity to hold both realities without splitting. We help the nucleus accumbens remain dopamine-activated in current connection rather than pre-grieving. You experience increased capacity for presence with the living person despite knowing loss is coming, grief that unfolds gradually rather than all at once, preservation of the relational connection rather than premature emotional withdrawal, and natural grief-processing that begins with the actual loss rather than before it occurs.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent & Identity
Teen Suicidal Ideation & Self-Harm - Adolescent Self-Injury & Suicide Risk
This could be your breakthrough. Let's do this!
Your adolescent has concluded that the world would be better without them, and their nervous system is actively generating action-plans to disappear. Teen suicidal ideation and self-harm occur when an adolescent experiences such profound psychological pain that death appears preferable to continued living, and self-harm (cutting, scratching, burning, etc.) becomes the mechanism to temporarily manage that pain. Suicidal adolescents are not attempting to "get attention"—they're experiencing genuine existential unbearability. Self-harm is often not suicidal-intent but rather an attempt to make emotional pain physical and thereby tolerable ("If I cut, I control the pain; I choose when to hurt; this physical sensation is manageable whereas emotional dysregulation is not"). Both self-harm and suicidal ideation indicate that the adolescent's current pain-management strategies have failed completely. Suicidality in adolescents often involves: untreated depression/trauma, experiencing rejection or social exclusion, feeling hopeless about future, perfectionism + recent failure, or family history of suicide.
The neurobiological mechanism: the ventromedial prefrontal cortex has entirely lost capacity to generate future-oriented thinking ("In one year, things might be different" is neurologically unavailable). Depression-related anhedonia has shut down dopamine-reward systems entirely—nothing feels good, nothing feels worth living for. The amygdala is in permanent threat-state, generating constant suffering-signals. Chronic pain from emotion is perceived through the anterior insula like chronic physical pain. The orbitofrontal cortex has lost value-weighting of life-sustaining activities. The anterior cingulate cortex generates unbearable emotional distress without matching coping capacity. The serotonin system is deregulated (depression pathway). Self-harm temporarily activates endogenous opioid systems, providing brief relief. Suicidal ideation represents the belief that pain can only end through death.
Our technique begins with immediate crisis intervention and safety-planning (suicidality at any level requires immediate professional emergency intervention). We rebuild the ventromedial prefrontal cortex's capacity for future-oriented thinking and hope by addressing the specific circumstances generating hopelessness. We treat underlying depression/trauma/rejection. We develop actual pain-management alternatives to self-harm. We restore oxytocin-bonding through suicide prevention collaborative and genuine peer/family support. The anterior insula learns that emotional pain is manageable. The nucleus accumbens regains capacity to sense dopamine-reward. The adolescent experiences restored will-to-live, decreased suicidal ideation, cessation of self-harm, and integration of the pain that generated the self-injury impulse.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Identity Development & Self-Discovery - Teen Identity Confusion
This could be your breakthrough. Let's do this!
Your adolescent nervous system is literally reconstructing itself, and the person you were yesterday no longer exists. Adolescent identity development issues occur when a teen navigates the profound neurobiological and social transformation of identifying who they are—separate from their parents, distinct in their beliefs and preferences, and differentiated in their social roles. Identity confusion manifests as frantic searching across social groups, ideologies, and values; terror of being "nobody"; desperate adoption of surface identities without authentic integration; or paralysis in the face of the infinite possibilities of who to become. The anterior cingulate cortex (self-referential thinking) and medial prefrontal cortex undergo massive recalibration during adolescence. The reward circuits become hypersensitive to peer validation and social status, making identity feel contingent on external approval rather than authentic self-discovery.
The neurobiological mechanism: the prefrontal cortex undergoes pruning and myelination during adolescence, losing its childhood efficiency while building more complex circuits. The medial prefrontal cortex (self-concept) literally doesn't know who the adolescent is anymore because the neural patterns that defined childhood self are being dismantled. The amygdala becomes hypersensitive to social evaluation and rejection during this window. The nucleus accumbens becomes intensely dopamine-responsive to peer approval and status, creating an addiction-like dependence on social validation. The ventromedial prefrontal cortex fails to provide coherent self-worth independent of external feedback. The teen experiences existential terror about identity ("Who am I if I'm not what my parents wanted, what my friends expect, or what society demands?").
Our technique stabilizes the medial prefrontal cortex during its reconstruction by anchoring the adolescent to their authentic values rather than reactive social performance. We help the teen separate identity-exploration from identity-desperation. The ventromedial prefrontal cortex learns to generate intrinsic self-worth independent of social approval, while the nucleus accumbens recalibrates to find reward in authentic self-expression rather than peer validation-seeking. The amygdala ceases treating identity-differentiation as social threat. The adolescent experiences genuine self-discovery rooted in values alignment rather than frantic persona-cycling, and the capacity to maintain authentic identity even when it differentiates from peer groups.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Angst & Oppositional Defiance - Teen Autonomy Rebellion
This could be your breakthrough. Let's do this!
Your adolescent cannot tolerate a single parental directive without experiencing it as an existential threat to their emerging autonomy. Adolescent angst and oppositional defiance occur when a teen's nervous system is hyperresponsive to perceived control, authority, and limitation—not because they disagree with the rule, but because parental authority itself feels like suffocation. The oppositional response is neurologically automatic: whenever an adult asserts authority, the amygdala triggers a threat-response and the orbitalfrontal cortex generates an automatic rejection impulse. The teen may disobey even when the consequences are severe and the restriction is reasonable, because the amygdala's threat-response to authority overrides rational evaluation. Oppositional defiance creates relational warfare between teen and parents, where every interaction becomes a power struggle.
The neurobiological mechanism: the dorsolateral prefrontal cortex undergoes massive reorganization during adolescence, shifting from external authority-reliance to internal autonomy. The amygdala becomes hyperactive to any signal of parental control or restriction. The orbitalfrontal cortex—responsible for evaluating social value and social hierarchy—becomes confused about authority: the neural circuits that encoded "parent as protector" are dismantling, while new circuits are forming that code parent authority as threatening to the emerging autonomous self. The nucleus accumbens becomes dopamine-sensitive to acts of defiance and rule-breaking, making rebellion neurochemically rewarding. The medial prefrontal cortex encodes compliance as loss of self. The anterior cingulate cortex (conflict monitoring) becomes hyperactive—every parental request is neurologically coded as conflict rather than care.
Our technique decouples authority from threat in the adolescent's amygdala, separating legitimate safety-setting from arbitrary control. We rebuild the distinction between healthy autonomy-seeking and defensive rebelliousness. The orbitalfrontal cortex learns that accepting help/guidance is not loss of autonomy. The prefrontal cortex regains capacity to evaluate rules rationally ("Is this reasonable?" rather than "Does this feel like control?"). The teen develops capacity for genuine autonomy—authentic choice-making rather than reactive defiance. Relationships with parents transform from power-struggles into collaborative problem-solving where the teen's voice and autonomy are respected within reasonable safety parameters.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Victim Identity & Learned Helplessness - Teen Powerlessness
This could be your breakthrough. Let's do this!
Your adolescent's nervous system has locked into the conclusion that nothing they do matters, that all outcomes are determined by external forces, and that effort is pointless. Adolescent victim identity and learned helplessness occur when a teen experiences repeated situations where their actions have no impact on outcomes, and this generates a generalized belief that they are powerless, that the world is hostile and uncontrollable, and that victimhood is their core identity. The learnt helplessness extends across all domains—the teen doesn't try in school because "What's the point?", doesn't attempt relationships because "I'm unlovable," doesn't take self-care actions because "Nothing helps." The victim identity becomes the primary self-concept—the teen organizes their entire self-narrative around oppression, injustice, and powerlessness.
The neurobiological mechanism: the ventromedial prefrontal cortex encodes powerlessness—the circuits that would normally generate agency and self-efficacy have been disabled by repeated failure. The anterior insula becomes hyperactive to experiences of pain/injustice, amplifying the sense of victimhood. The amygdala becomes locked in threat-response because the nervous system has concluded the world is unsafe and uncontrollable. The nucleus accumbens becomes depleted of dopamine—there's no reward-anticipation for effort because effort hasn't produced positive outcomes. The dorsolateral prefrontal cortex loses capacity for goal-directed behavior (if effort doesn't work, why try?). The medial prefrontal cortex encodes the victim identity as core self. The anterior cingulate cortex stops monitoring for change—the nervous system expects helplessness.
Our technique rebuilds agency by creating experiences where the adolescent's actions DO produce outcomes. We help the teen distinguish between actual injustice (valid and potentially worth addressing) and learned helplessness (a neural pattern that's treatable). The ventromedial prefrontal cortex relearns self-efficacy through small, achievable experiences of agency. The nucleus accumbens regains dopamine-responsiveness to successful action. The amygdala begins to recognize situations where the teen DOES have capacity to influence outcomes. The adolescent develops restored sense of agency, capacity to take protective action on their own behalf, ability to distinguish between unchangeable circumstances and those within their control, and gradual shift from victim-identity toward resilience-identity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Risk-Taking, Impulsivity & Executive Dysfunction - Reckless Behavior & Distress-Driven Impulse Control
This could be your breakthrough. Let's do this!
Your adolescent's nervous system either uses risky behavior to manage unbearable emotional distress OR lacks the executive capacity to inhibit dangerous impulses—or both. Adolescent risk-taking and impulsivity span two neurobiological mechanisms that frequently co-occur: (1) distress intolerance where the adolescent deliberately seeks adrenaline-surge to override emotional pain, and (2) executive immaturity where the developing prefrontal cortex cannot inhibit amygdala-driven impulses in real-time situations. Risk behaviors range from intentional thrill-seeking designed to regulate dysphoria, to impulsive consequence-blindness, to escalating cycles where both mechanisms reinforce each other. The adolescent may engage in reckless driving, extreme sports, dangerous peer activities, unprotected sex, fights, or other high-risk behaviors that generate either immediate dopamine-relief or immediate thrill-reward. Genuine emotional regulation capacity fails to develop when risk-taking "solves" the distress problem, and executive inhibition remains weak until the prefrontal cortex finishes maturational development (often not until the mid-20s).
The neurobiological mechanism involves both dysregulated emotion-processing systems AND immature executive development. The insula (interoceptive awareness of emotional/bodily states) becomes hyperresponsive to emotional pain, making distress feel intolerable. The ventromedial prefrontal cortex fails to develop capacity to tolerate emotional experience—it immediately sends distress-alarm to the amygdala, which demands immediate action to stop the feeling. Simultaneously, the dorsolateral prefrontal cortex (executive function, consequence-evaluation, impulse-inhibition) is the brain region that develops LAST in adolescence. The ventromedial prefrontal cortex is still developing and remains weak compared to the amygdala and nucleus accumbens. When the amygdala fires in response to exciting/dangerous situation or intense emotional pain, it overwhelms whatever prefrontal capacity exists to "pump the brakes." The nucleus accumbens becomes dopamine-sensitized to adrenaline, thrill, and immediate reward—the adolescent's reward system has been trained to depend on high-risk stimulation and becomes additively sensitized as the teen escalates danger-level to maintain the dopamine surge. The anterior cingulate cortex fails to develop adequate emotion-acceptance capacity and conflict-monitoring. The white-matter connectivity between prefrontal regions and limbic regions is still being myelinated—the "highway" for executive control hasn't fully formed yet. Risk-taking becomes neurochemically addictive: whether driven by distress-regulation or impulsive reward-seeking, the behavior itself generates dopamine that reinforces continued escalation.
Our technique addresses both underlying mechanisms: rebuilding distress-tolerance so the adolescent's nervous system can process emotional experience without generating existential panic, while simultaneously building inhibitory capacity and external structure that supports the still-developing prefrontal systems. The insula learns to process emotional experience without generating existential panic. The ventromedial prefrontal cortex develops capacity to hold emotional experience without demanding immediate escape AND learns to weight short-term impulse-reward against long-term consequences more effectively. We teach vagal regulation skills and explicit decision-making strategies that activate the parasympathetic nervous system as alternatives to adrenaline-seeking. The nucleus accumbens gradually recalibrates to find dopamine-reward in genuine emotion regulation, healthy goal-pursuit, and social connection rather than only in risk-taking. The dorsolateral prefrontal cortex develops functional inhibitory capacity through practice, and we support environmental structure that reduces the need for impulse-inhibition while development is ongoing. The anterior cingulate cortex develops emotion-acceptance capacity and genuine conflict-monitoring. Parents/caregivers learn to provide structure, limits, and consequences that support the developing executive system. The adolescent experiences increased distress-tolerance, decreased catastrophic impulsive choices, improved real-world outcomes, capacity to process difficult emotions without dangerous coping, safer mechanisms for emotion-regulation, and freedom from the escalating danger-spiral.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Sexual Identity Exploration & Social Dysphoria - Teen Gender/Sexual Confusion
This could be your breakthrough. Let's do this!
Your adolescent's nervous system is screaming that something is mismatched between their internal sense of self and the body/sexuality society assigned them. Adolescent sexual identity exploration and social dysphoria arise when a teen questions their sexual orientation, gender identity, or both, and experiences distress about the mismatch between internal identity and external presentation/expectations. This is distinct from simply exploring sexuality—dysphoria involves mental suffering, social alienation, fear of rejection, difficulty integrating multiple identity-aspects, and the amygdala's terror-response to being revealed as "abnormal." The teen may dissociate from their body, experience dysphoric panic about puberty changes, avoid peer interaction due to identity-mismatch terror, or desperately perform a false identity while their authentic identity remains hidden.
The neurobiological mechanism: the anterior insula (body-awareness and aversion) becomes hyperactive in dysphoria—the teen's own body generates distress signals. The medial prefrontal cortex encodes the authentic sexual/gender identity as dangerous ("If I reveal this, I will be rejected, harmed, or abandoned"). The amygdala becomes hyperresponsive to social mirroring of assigned identity ("When they refer to me as 'she/he,' my nervous system codes it as a threat to my authentic self"). The ventromedial prefrontal cortex fails to generate self-worth because societal messages code the authentic identity as unworthy. Stress hormones remain chronically elevated (cortisol) due to the constant effort of identity-hiding. The reward circuits (nucleus accumbens) become dopamine-depleted around authentic identity expression because every expression-attempt has been punished, shamed, or rejected.
Our technique targets the insula's dysphoric encoding of the body and rebuilds safety around authentic sexual/gender identity expression. The amygdala learns that revealing authentic identity can be safe—not all humans respond with rejection or violence. The medial prefrontal cortex codes authentic identity as coherent self rather than shameful secret. The ventromedial prefrontal cortex rebuilds intrinsic self-worth not contingent on sexual/gender conformity. The teen develops capacity to explore and integrate sexual/gender identity at a pace that feels safe, to find community with others who share similar identity experiences, and to live with decreasing dysphoria and increasing authentic presence.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Adolescent Social Mimicry & Identity Diffusion - Teen Identity Instability
This could be your breakthrough. Let's do this!
Your adolescent is a different person in every social context, and internally feels completely fragmented with no coherent sense of authentic self. Adolescent social mimicry and identity diffusion occur when a teen becomes excessively skilled at reading social contexts and performing the identity that each context requires, but never develops an internal sense of who they authentically are. The mimicry may be adaptive survival (learned in families where identity-authenticity was unsafe), may be rooted in peer-dependence where identity feels contingent on group-approval, or may be protective against rejection (if no one knows the real you, no one can reject the real you). As a result, the teen experiences: emptiness and internal void, inability to know their own preferences/values, constant shapeshifting across contexts, chronic dissociation or depersonalization, and the exhausting labor of maintaining multiple authentic-seeming personas.
The neurobiological mechanism: the medial prefrontal cortex (self-referential processing and self-concept) has never developed authentic self-representation. Instead, it has developed expert mirror-neuron capacity and social-cognitive mapping—the teen can read others' expectations perfectly but has no template for authentic self. The ventromedial prefrontal cortex generates self-concept that is entirely dependent on reflected appraisals (who do people expect me to be?). The anterior insula becomes dysregulated by the constant gap between performed self and absent authentic self. The nucleus accumbens becomes dopamine-dependent on social approval of the performed identity. The anterior cingulate cortex experiences chronic conflict without resolution (performing vs. authentic). Dissociation and depersonalization may accompany the chronic identity-fragmentation.
Our technique helps the medial prefrontal cortex develop authentic self-representation grounded in values, preferences, and genuine emotional responses rather than external-approval-seeking. We support the teen in tolerating the social risk of authenticity ("What if people don't like my real self?"). The ventromedial prefrontal cortex develops intrinsic self-worth not dependent on performed identity or approval. The anterior insula recalibrates to recognize that authenticity involves both acceptance and appropriate rejection (some people won't like you—that's okay). The nucleus accumbens learns to find dopamine-reward in authentic connection rather than wide-audience approval. The adolescent develops coherent, stable sense of authentic self, decreased identity-fragmentation, capacity to bring authentic self into social contexts, and the relief of genuine connection based on real identity rather than performed persona.
Related conditions: This teen-specific social mimicry and identity diffusion is developmentally related to the broader Self-Esteem & Identity Issues condition in adults, and identity confusion is tied to Adolescent Sexual Identity Exploration and sexual/gender development.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Emo Subculture & Emotional Expression - Alternative Identity Adoption
This could be your breakthrough. Let's do this!
Your adolescent found a tribe that finally allows their intense emotions to be normal instead of pathological. Teen emo subculture and emotional expression issues occur when an adolescent adopts an alternative identity and aesthetic (emo, goth, punk, etc.) as both a genuine expression of their emotional intensity and, simultaneously, a defensive identity-container that keeps vulnerability controlled and emotions performative. The emo subculture offers permission for emotional depth and intensity that mainstream teen culture penalizes. However, the adoption can become problematic when it's rooted primarily in distress-performance rather than authentic expression, when it forecloses other identity development, or when it becomes a barrier to developing genuine emotional regulation capacity. The teen experiences validation within the subculture, but may have difficulty integrating emotional depth with other identity aspects or developing genuine coping that doesn't depend on subcultural performance.
The neurobiological mechanism: the anterior insula (emotional awareness) becomes activated and validated in subcultures that welcome emotional intensity—a relief from mainstream teen culture's demand for emotional suppression. The medial prefrontal cortex can finally code intense emotion as acceptable rather than pathological. However, if the subculture-adoption is primarily defensive, the ventromedial prefrontal cortex fails to develop intrinsic emotional regulation. The amygdala becomes dependent on external subcultural validation to manage emotion. The orbitofrontal cortex may code mainstream identity-spaces as permanently unsafe, limiting the teen's social flexibility. The nucleus accumbens becomes reward-dependent on subcultural status and aesthetics rather than genuine emotional skill-building.
Our technique supports the genuine aspects of emotional expression while building intrinsic emotional regulation independent of subcultural performance. We help the adolescent distinguish between authentic emotional intensity (valid and worth preserving) and defensive emotional performance (limiting and unsustainable). The ventromedial prefrontal cortex develops genuine emotion-regulation skills. The teen experiences the capacity to express authentic emotional depth in multiple contexts (not just within the subculture), to integrate emotional intensity with other identity aspects, and to make identity-choices from authentic preference rather than defensive subcultural dependence.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Crisis & Survival Behaviors - Adolescent Acute Distress Response
This could be your breakthrough. Let's do this!
Your adolescent is in neurological emergency—their nervous system has concluded that the current situation is unsustainable and survival-action is required immediately. Teen crisis and survival behaviors occur when an adolescent in acute psychological distress engages in urgent action to escape the crisis: runaway attempts, suicide attempts, aggressive crisis-seeking (calling police on themselves), suicidal communication, substance overdose, cutting escalation, or other dramatic crisis-interventions. The crisis behavior is not calculated manipulation—it's genuine neurological emergency. The amygdala has concluded that current circumstances are unsustainable, the ventromedial prefrontal cortex can't generate solutions, and the only option remaining is emergency-action. Crisis behaviors are usually preceded by a period of increasing distress where normal coping has failed, where parental/professional support has been unavailable or ineffective, and where the adolescent feels completely trapped.
The neurobiological mechanism: the amygdala is in maximum threat-response (this is survival-mode, not ordinary fear). The ventromedial prefrontal cortex is completely offline—the teen can't access problem-solving or perspective. The anterior cingulate cortex is hyperactive but generating only distress-signals with no solutions. The insula is generating intense bodily distress-signals (everything feels unbearable). The dorsolateral prefrontal cortex is unable to access longer-term thinking or memory of previous survival. Suicidal ideation or crisis-action feels like the only solution because all other options have been neurologically foreclosed by the intensity of threat-perception. The nervous system has concluded: "I cannot survive this."
Our technique begins with immediate stabilization and safety (this is genuine emergency intervention requiring crisis-professional involvement). We recalibrate the amygdala's threat-assessment by addressing the triggering circumstances and providing actual safety/support. The ventromedial prefrontal cortex regains problem-solving capacity as the acute threat reduces. The anterior cingulate cortex begins to generate genuine options rather than only distress-signals. We address the underlying conditions that generated the crisis (family trauma, peer crisis, academic breakdown, etc.) and build sustainable coping capacity. The adolescent experiences decrease in acute suicidal/crisis ideation, restored problem-solving capacity, safety-planning and genuine support systems, and development of sustainable coping that makes crisis-behaviors unnecessary.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Gang Involvement & Tribalism - Adolescent Group Belonging
This could be your breakthrough. Let's do this!
Your adolescent found a family that finally cares, finally provides status and protection, finally makes them feel powerful—and that family is actively escalating toward violence. Teen gang involvement and tribalism occur when an adolescent with a fundamental belonging-wound finds that the gang meets the need: the gang provides clear identity ("You are a member"), clear purpose ("You protect your territory and brothers"), clear status hierarchy (you work up), and fierce loyalty structure. However, gang involvement locks the adolescent into violence, criminality, drug economy participation, and mortal danger. The amygdala becomes group-synchronized with gang violence-response, the reward system becomes dependent on gang-status dopamine, and the prefrontal cortex becomes unable to evaluate exit-consequences because gang loyalty is coded as more important than survival. The teen may intellectually recognize gang danger but remain neurologically bound to the group.
The neurobiological mechanism: the adolescent brain's need for belonging and status is neurologically intense. The nucleus accumbens becomes hypersensitive to gang-status dopamine (becoming a higher-ranking member, earning respect, gaining territory). The amygdala becomes synchronized with the group's threat-response—the teen can't generate independent threat-evaluation because they've internalized the gang's collective amygdala. The medial prefrontal cortex encodes gang-membership as core identity. The ventromedial prefrontal cortex becomes unable to generate self-worth independent of gang-status. The orbitofrontal cortex becomes locked into the gang's value-hierarchy. Violence becomes normalized through repeated exposure and becomes personally normatized by the amygdala (threat-response to rival gangs becomes authentic perceived threat rather than socially-constructed threat).
Our technique begins by acknowledging that the gang met a real need (belonging, status, protection) and that exiting requires developing these needs through non-violent channels. We help the adolescent disconnect amygdala-synchronization with the group through trauma processing of gang-violence exposure. The ventromedial prefrontal cortex develops intrinsic self-worth not dependent on gang-status. The nucleus accumbens learns to find dopamine-reward in school achievement, healthy relationships, genuine mentorship, and other status-pathways. The prefrontal cortex regains capacity for independent threat-evaluation and exit-planning. The adolescent develops capacity to exit gang involvement, access mentorship and legitimate opportunity, rebuild relationships outside gang, and develop identity that doesn't depend on violence or criminal participation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Neurodevelopmental & Communication
General Neurodevelopmental Issues
This could be your breakthrough. Let's do this!
Your nervous system developed with atypical wiring patterns that create functional challenges across multiple domains. Whether coordination, attention, social processing, or motor planning, the developing brain took a different path. Neurodevelopmental issues encompass diverse conditions including various learning disabilities, motor coordination difficulties, speech/language disorders, and social-communication differences that emerge during development and cause significant functional or educational impairment despite adequate environmental support and opportunity.
The neurobiological mechanisms vary across specific neurodevelopmental conditions but generally involve atypical neural development during critical periods—whether through genetic factors, prenatal influences, birth complications, or early environmental factors that alter typical neural pathway development. This results in brain systems that process information differently, often requiring more effort in affected domains despite average or above-average overall capability. Anxiety often co-occurs or develops secondarily as individuals encounter repeated difficulty in affected domains, creating additional functional challenges.
Our technique identifies and recalibrates the specific neural pathway differences through targeted neurodevelopmental intervention. We enhance the efficiency of atypical neural pathways and reduce secondary anxiety that compounds functional difficulty. Your brain's atypical wiring becomes an asset rather than a limitation, processing efficiently through its unique pathways. You experience functional improvements in affected domains and restored confidence in your capabilities.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.ADHD - Attention Deficit Hyperactivity Disorder
This could be your breakthrough. Let's do this!
Your prefrontal cortex is shouting for attention. Anxiety is jamming the signal. Attention-Deficit/Hyperactivity Disorder (ADHD) is a neurodevelopmental condition affecting the brain's regulation of attention, impulse control, and executive functions like planning, organization, and task initiation. Individuals with ADHD often struggle with sustained attention, time management, and follow-through on tasks, which can significantly impact academic achievement, employment, and self-esteem. While ADHD has a strong neurobiological basis, it is frequently complicated by secondary anxiety and emotional dysregulation.
The contribution of anxiety to ADHD symptomatology is profound and often underrecognized—anxiety creates a 'noise' in the prefrontal cortex that exacerbates executive dysfunction. When the limbic system perceives tasks as threats or the individual is in a state of hypervigilance, executive function becomes severely compromised, leading to paralysis when trying to initiate or complete tasks. This creates a cruel paradox where anxiety about not accomplishing tasks further impairs the very executive function needed to accomplish them. Emotional dysregulation amplifies task avoidance, creating downward spirals of lost time and lost opportunity.
Our technique targets the anxiety infrastructure that compounds ADHD impairment. By reducing threat-sensitivity and reinstating executive capacity, you access striking improvements in focus, task completion, time management, and emotional regulation. This isn't cognitive training or behavioral management. It's targeted recalibration of the limbic hyperactivity that hijacks prefrontal function. Participants experience measurable improvements in academic and occupational functioning within weeks. Your executive function emerges when anxiety stops overriding it.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
ASD - Autism, Asperger's and Autistic Spectrum Disorder
This could be your breakthrough. Let's do this!
Your nervous system processes information in its own way. Comfort comes from understanding and honoring that, not fighting it. Autism Spectrum Disorder (ASD) is a neurodevelopmental condition characterized by differences in social communication, repetitive behaviors or interests, and sensory processing. Individuals on the autism spectrum experience the world in distinct ways, with strengths in areas like pattern recognition, attention to detail, and focused interest, alongside challenges in areas like social reciprocity and sensory regulation. ASD is not a disorder to be cured but a neurological difference that deserves understanding and accommodation.
While autism itself is a neurodevelopmental variation rather than an anxiety disorder, comorbid anxiety is extremely common in autistic individuals, particularly as they navigate social demands and environmental expectations. Anxiety heightens amygdala reactivity, leading to sensory overload where the filtering mechanisms that allow selective attention become overwhelmed. This overwhelm often leads to increased reliance on repetitive behaviors or 'stimming' to self-regulate an overstimulated nervous system, creating cycles of withdrawal and further social isolation.
Our technique isn't about 'curing' autism or making you more neurotypical. It's about helping you manage anxiety-driven sensory dysregulation that often accompanies autism in a non-autistic world. By reducing anxiety-driven amygdala hyperactivity and improving nervous system regulation capacity, we help you feel more comfortable in your own systems. This allows genuine engagement in social and occupational activities while maintaining authentic autistic identity and neurodiversity strengths. You access your neurological gifts without the chains of anxiety.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
DCD - Dyspraxia and Developmental Coordination Disorder
This could be your breakthrough. Let's do this!
Your body knows what to do. Your nervous system is just broadcasting too much static to let it happen. Developmental Coordination Disorder (DCD), also known as dyspraxia, is a neurodevelopmental condition affecting the motor planning and coordination pathways, leading to physical clumsiness, difficulty with complex movement sequences, and impaired athletic ability. Individuals with DCD may struggle with seemingly simple tasks like tying shoes, catching a ball, or handwriting, while having normal intelligence and understanding of what they need to do. This disconnect between intention and motor execution is frustrating and often leads to social shame, bullying, and secondary anxiety.
The cerebellum and basal ganglia work together to create the fluid, coordinated movements we take for granted—they must perfectly time the contraction of hundreds of muscles with incredible precision. Anxiety disrupts the motor planning pathways between the cerebellum and cortex, causing increased physical clumsiness and difficulty with complex sequence movements. When anxiety is present, these motor coordination systems become even more dysregulated, leading to increased tension, tremors, and further deterioration of movement quality. The motor coordination circuitry becomes jammed by limbic noise.
Our technique restores smooth motor planning by reducing anxiety and targeting the cerebellum-cortex communication pathways through targeted recalibration. We diminish the neurological noise that jams coordination. Movements become fluid and automatic as planning and execution synchronize. This isn't physical therapy or practice. It's targeted recalibration of how the nervous system communicates movement instruction. You report that as anxiety decreases, physical movements become more fluid, athletic performance improves, and handwriting becomes readable.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.SPD - Sensory Processing Disorder
This could be your breakthrough. Let's do this!
Your sensory system's volume dial got stuck on full blast. It's time to restore the dynamic range. Sensory Processing Disorder is characterized by difficulties in detecting, interpreting, or responding appropriately to sensory information from the body or environment, leading to difficulty functioning in daily life. Individuals with SPD may be hypersensitive to stimuli like touch, sound, or light and experience them as painful or overwhelming, or may be hyposensitive and fail to register sensory input. This can result in hyperactivity seeking stimulation, social withdrawal, poor motor coordination, or emotional dysregulation that significantly restricts daily functioning and social participation.
Anxiety interacts with sensory processing in ways that significantly amplify hypersensitivity symptoms—the amygdala, when in a threat-detection state, lowers the threshold for what sensory input is perceived as aversive or dangerous. Anxiety places the brain in a state of hyper-vigilance, lowering the sensitivity threshold for sensory input and causing the limbic system to interpret neutral stimuli as physically painful. A gentle touch may feel irritating, routine sounds may seem intolerable, or ordinary visual environments may feel overwhelming when anxiety has heightened the salience of sensory information. The sensory gates malfunction under threat conditions.
Our technique restores normal sensory gating by reducing threat-sensitivity and recalibrating the amygdala's threat response to sensory stimuli through targeted creative intervention. Hypersensitivity recedes substantially as your nervous system stops interpreting neutral sensory input as dangerous. This isn't occupational therapy or gradual habituation. It's targeted recoding of sensory threat perception. You experience striking improvements in sensory tolerance and comfort, engaging fully in social, occupational, and recreational activities.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Dyslexia - Reading Disorder
This could be your breakthrough. Let's do this!
Your brain processes written language through atypical pathways that make reading laborious and error-prone. The phonological and orthographic pathways are not optimally integrated. Dyslexia is a specific learning disability affecting the ability to read, characterized by difficulty with decoding, word recognition, reading fluency, and/or spelling despite normal intelligence and adequate instruction. Individuals with dyslexia often read slowly and laboriously, make reading errors, avoid reading tasks, and experience profound academic stress. Undiagnosed dyslexia often leads to shame about intelligence despite having average or above-average cognitive abilities.
The neurobiological mechanism involves atypical connectivity between the visual cortex (recognizing written forms) and the phonological processing centers (Wernicke's area, left temporo-parietal region). The brain's typical pathway from visual letter recognition to phonological mapping becomes less efficient, requiring increased effort and cognitive resources to decode written words. Reading requires slow, effortful sounding-out rather than automatic recognition. Additionally, anxiety about reading performance activates the amygdala, further impairing the already-difficult decoding process by consuming working memory and increasing reading errors in a stress-performance feedback loop.
Our technique optimizes the visual-phonological integration pathways and reduces reading-related anxiety through targeted limbic and visual processing intervention. We enhance the neural coordination between visual recognition and phonological access. Your reading becomes more fluent and automatic as the visual-phonological pathways synchronize. This isn't reading tutoring or more practice. It's recalibration of how the brain integrates visual letter forms with sound. You experience faster reading speed, improved accuracy, and restored willingness to engage with written material.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Dyscalculia
This could be your breakthrough. Let's do this!
Your brain processes numbers just fine. When anxiety isn't hijacking your parietal cortex, that changes. Dyscalculia is a specific learning disability affecting the ability to understand numbers and learn math facts and skills, despite normal intelligence and adequate instruction. Individuals with dyscalculia struggle with number sense, basic arithmetic operations, and mathematical reasoning, which can severely limit career opportunities and lead to pervasive shame about their cognitive abilities. Importantly, dyscalculia is not a result of insufficient effort or poor instruction, but reflects underlying differences in how the brain processes numerical information.
Math-related anxiety is endemic in dyscalculia and plays a significant amplifying role in academic difficulties. Math-related anxiety activates the amygdala while suppressing activity in the parietal lobes where numerical processing occurs, literally blocking the brain's ability to process numerical information at the moment it's needed most. When students with dyscalculia encounter math, anxiety surges, their brain's numerical processing capacity is suppressed, they struggle further, and anxiety escalates in a feedback loop of avoidance and failure. Anxiety creates a direct cognitive block.
Our technique reduces math-related anxiety by recalibrating threat perception and restoring parietal lobe function through targeted creative intervention. We dissolve the anxiety-driven suppression of numerical processing circuits. Your brain regains access to its intact number sense and mathematical capability. This isn't tutoring or more math practice. It's targeted recalibration of the anxiety-amygdala-number processing loop. You experience that improvements in math anxiety translate directly into improvements in math performance, confidence, and willingness to engage.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.General Communication Issues
This could be your breakthrough. Let's do this!
Your nervous system struggles with the complex coordination required for clear communication. Whether timing, word selection, or social-emotional attunement, authentic communication became difficult. General communication issues encompass diverse difficulties with verbal or nonverbal communication including stuttering, unclear speech intelligibility, difficulty with conversational flow, poor listening skills, or lack of attunement to communication partner's perspective. These create significant social and occupational difficulties despite potentially intact underlying cognitive or language capability.
The neurobiological mechanisms vary across communication issues but often involve coordination problems between language production and motor execution systems (stuttering), auditory processing difficulties (listening), social-emotional processing differences (conversational attunement), or attention/executive deficits that affect real-time communication management. Anxiety often develops secondarily where individuals become hyperaware of communication difficulties, leading to avoidance of communication, which further impairs practice-based improvement.
Our technique recalibrates the specific communication system disruption through targeted neural intervention. We improve neural coordination in affected communication systems and reduce secondary anxiety that compounds difficulty. Your communication becomes more fluid, accurate, and socially effective. This isn't speech therapy or communication coaching. It's targeted recalibration of the neural systems generating communication difficulty. You experience improved communication effectiveness and restored confidence in social and professional communication.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Aphasia - Language Disorder
This could be your breakthrough. Let's do this!
Your language system became disrupted and now words don't flow as they used to. Language access became blocked or slowed. Aphasia is an acquired language disorder typically resulting from stroke, brain injury, or neurological disease, characterized by difficulty with language production (expressive aphasia), language comprehension (receptive aphasia), or both. Individuals with aphasia may experience word-finding difficulty, trouble understanding speech, reading/writing problems, or complete language loss depending on the brain regions affected. Aphasia creates profound communication challenges, social isolation, and often depression secondary to language loss.
The neurobiological mechanism involves damage or disruption to language-dominant brain regions typically in the left hemisphere, including Broca's area (language production), Wernicke's area (language comprehension), and connecting pathways. The specific language difficulties depend on the lesion location: Broca's aphasia involves speech production difficulty while comprehension remains; Wernicke's aphasia involves comprehension difficulty while speech production continues but becomes nonsensical. The remaining intact brain regions may gradually compensate through neuroplasticity, though recovery depends on damage extent and time since injury. Anxiety about communication often compounds language difficulty.
Our technique facilitates neural plasticity and language pathway reorganization through targeted language and limbic intervention. We engage compensatory neural pathways and reduce anxiety about communication. Your language access improves as the brain reorganizes function around the damage. This isn't speech therapy in the traditional sense. It's targeted facilitation of neural adaptation and language recovery. You can experience rapid language recovery and restored communication capacity, but individual results may vary depending on the lesion location.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Stuttering and Childhood-Onset Fluency Disorder
This could be your breakthrough. Let's do this!
Stuttering is a speech fluency disorder characterized by involuntary disruptions in the flow of speech, including repetitions of sounds or syllables, prolongations of sounds, or complete blocks where speech temporarily ceases. Far more than a simple speech impediment, stuttering often becomes deeply intertwined with anxiety and social fear, particularly during periods like adolescence when peer communication becomes central to social identity. The condition can significantly impact academic performance, employment opportunities, and psychological wellbeing when left unaddressed.
The mechanism linking anxiety to stuttering operates through disruption of the precise neural timing systems required for coordinated speech production. Social anxiety and performance stress activate limbic fight-or-flight responses that disrupt the fine motor coordination and timing between respiration, phonation, and articulation needed for fluent speech. The increased nervousness about stuttering itself becomes self-perpetuating, creating a vicious cycle where anxiety about speaking impairs speech even further, leading to increased blocks and repetitions.
Our research demonstrates that by breaking the hardened anxiety-stutter loop, individuals experience transformative improvements in speech fluency, often without traditional speech therapy. We dissolve the anxiety coding and replace it with synaptic patterns of courage that liberate smooth speech production. Motor systems access fluency swiftly, with participants experiencing substantial shifts in their speaking capability, confidence, and willingness to communicate fully in social and professional contexts.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Selective Mutism
This could be your breakthrough. Let's do this!
Your voice is locked in your throat by a false threat signal. It's time to find the off switch. Selective Mutism is an anxiety disorder in which individuals, typically children, are unable to speak in specific social situations despite being able to speak normally in other contexts, such as at home. This is not a choice or willful defiance, but rather an involuntary freezing response where the individual feels physically unable to produce speech despite desperately wanting to communicate. Selective mutism severely impacts academic performance, social relationships, and can lead to significant secondary anxiety and depression if not addressed.
The neurobiological mechanism involves a conditioned fear response where the amygdala perceives social interaction, particularly speaking to authority figures or in front of peers, as a life-threatening danger. The amygdala's threat assessment triggers a freezing response that physically prevents the vocal cords from operating in specific settings. This freezing response represents an ancient survival mechanism where immobility and silence were adaptive responses to predation, but which becomes maladaptive when triggered by social situations. The voice is literally held hostage.
Our technique shatters the selective mutism loop through targeted limbic reprogramming. We dissolve the social-threat perception and restore vocal freedom. The freezing response transforms and is replaced with genuine access to voice and authentic communication. This isn't gradual exposure or progressive talking. It's swift recalibration of the amygdala's social threat assessment. You access voice in social contexts at striking speed, moving from complete silence to authentic vocal power.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Dysgraphia
This could be your breakthrough. Let's do this!
Your hand could write beautifully if anxiety's stranglehold grip didn't paralyze your fine motor control. Dysgraphia is a specific learning disability affecting the ability to write, characterized by illegible handwriting, spelling difficulties, and problems with written expression despite normal intelligence and adequate instruction. Individuals with dysgraphia often write slowly, laboriously, and painfully, with poor letter formation and spatial organization on the page. The struggle to write often masks underlying knowledge and capability, leading to academic underperformance and secondary shame about writing abilities that follows them into adulthood.
Anxiety significantly exacerbates dysgraphia through multiple mechanisms involving fine motor control and cognitive load. Anxiety-induced sympathetic nervous system activation causes excessive grip tension and motor tremors, severely degrading the legibility and speed of physical writing. Additionally, anxiety consumes working memory capacity that could be devoted to organizing thoughts and translating them to written form, making writing even more effortful and slow. For students with dysgraphia, anxiety transforms an already-challenging task into something nearly impossible. The nervous system's fight-or-flight state became hardwired into writing.
Our technique restores a relaxed neuromuscular state and recalibrates working memory through targeted limbic recalibration. We reduce anxiety's grip on motor control and free cognitive resources for composition. Your hand becomes steady, writing speed increases, and thoughts flow onto paper. This isn't handwriting practice or more writing lessons. It's swift recalibration of anxiety's effects on fine motor and cognitive systems. As anxiety decreases, you can finally write without pain and your writing performance accurately reflects your knowledge and capability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Neurological & Movement Disorders
General Neurological Issues
This could be your breakthrough. Let's do this!
Your nervous system contains wiring patterns that create functional challenges across perception, sensation, or movement control. Whether from developmental differences, acquired injury, metabolic disruption, or neurodegenerative processes, the brain or nervous system generates symptoms that impair quality of life. General neurological issues encompass diverse conditions including various movement disorders, sensory processing variations, headache syndromes, and neurological symptoms that significantly impact functioning despite normal overall development or health status.
The neurobiological mechanisms vary across specific neurological conditions but generally involve atypical function in motor cortex, cerebellum, basal ganglia, sensory cortices, or other brain regions that generate symptoms specific to the affected system. Anxiety often co-occurs or develops as the secondary consequence when neurological symptoms create functional difficulty or social stigma. The amygdala may become sensitized to symptom-related threat or social threat, amplifying the subjective distress beyond the neurological basis alone.
Our technique addresses both the neurological symptom generation and secondary anxiety through targeted neural intervention. We enhance compensatory neural pathway function and reduce threat-sensitivity to symptom experience. Your brain regains maximum functional capacity given the neurological condition present. You experience improved functional capacity and reduced anxiety about neurological symptoms.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Migraines
This could be your breakthrough. Let's do this!
Migraines are a conversation between anxiety and your nervous system's pain-signaling center. And you can change the conversation. Migraines are a common neurological condition characterized by intense, debilitating headaches often accompanied by sensory disturbances, nausea, and heightened sensitivity to light and sound. Those affected by migraines experience not only the physical pain of the migraine attacks but also the anxiety and anticipation of future attacks, which can significantly limit activities and reduce quality of life.
The connection between anxiety and migraines is mediated through multiple pathways and the trigeminal nerve system, which is intimately connected to the emotional processing centers of the brain. Anxiety triggers a cascade of neurochemical changes including altered serotonin and dopamine levels, as well as muscular tension in the neck and shoulder region that activates the trigeminal nerve system. This activation often leads to more frequent and intense migraine attacks in susceptible individuals, creating a feedback loop where worry about migraines increases their likelihood of occurrence.
Our technique targets the anxiety-pain signaling loop through conscious reprogramming of the limbic system and nervous system's pain interpretation. We identify the specific amygdala hijacks and catastrophic beliefs that trigger migraine cascade, then rewire the threat response and pain sensitivity. This is not pain management or talking about stress. It is precision recalibration of how your nervous system interprets signal and generates response. Migraine frequency and intensity shift markedly.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Chronic Inner Ear Conditions - Vertigo, Tinnitus and Dizziness
This could be your breakthrough. Let's do this!
Some inner ear conditions begin as physical events and then remain active because the brain learns to treat ordinary vestibular or auditory signals as ongoing threat. This entry is for chronic inner-ear-related syndromes that are strongly shaped by stress, hypervigilance, and limbic looping. That includes Persistent Postural-Perceptual Dizziness (PPPD), chronic subjective dizziness, residual dizziness after vestibular neuritis or labyrinthitis, stress-amplified vertigo, tinnitus that has become threat-coded, auditory hypervigilance, and similar chronic vestibular-auditory patterns where the original event may have healed but the nervous system is still acting as if danger is present. People in this state often experience rocking, swaying, motion sensitivity, fear of falling, visually induced dizziness, ringing or buzzing in the ears, sleep disruption, concentration problems, and constant scanning for the next flare.
The neurobiological mechanism often involves a reciprocal loop between the vestibular system, auditory salience networks, and the limbic system. Once the amygdala classifies internal signals of motion, imbalance, ear noise, or sensory instability as dangerous, the brain allocates more attention and threat chemistry to them. Cortisol and adrenaline increase nervous system gain. The vestibular cortex, insula, attentional networks, and auditory pathways become more reactive. Fear of dizziness can generate more dizziness. Fear of tinnitus can make the sound feel louder and more intrusive. Habituation is blocked because the nervous system keeps flagging the signal as urgent instead of background. Over time, the problem becomes not only the original sensation but the brain's learned habit of monitoring and amplifying it.
Our technique targets the limbic amplification that keeps these chronic inner-ear-related conditions alive after the original trigger. By reducing amygdala hijacks, restoring prefrontal regulation, and allowing habituation to resume, the nervous system stops over-interpreting minor balance or auditory signals as emergencies. Neural sensitivity decreases, signal salience drops, and the chronic stress-symptom loop begins to dissolve. This is not a substitute for medical workup, and it does not claim to fix structural conditions that require ENT, neurologic, surgical, infectious, or metabolic treatment. It is designed for chronic vestibular-auditory conditions that are clearly stress-reactive and functionally amplified. It does not cover clearly structural or urgent conditions such as acoustic neuroma, cholesteatoma, active Ménière's disease requiring medical management, or other inner-ear disorders where the primary issue is not a stress-amplified nervous-system loop. When the amygdala stops broadcasting instability and alarm, the brain can relearn steadiness, filtering, and calm.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Epilepsy and Seizure Disorders
This could be your breakthrough. Let's do this!
Your nervous system's electrical cables are misfiring under stress. It's time to restore reliable current flow. Epilepsy is a neurological disorder characterized by a predisposition to recurrent seizures, which are sudden, uncontrolled electrical discharges in the brain leading to physical convulsions, altered consciousness, or other distinctive experiences. Individuals with epilepsy live with the constant threat of unpredictable seizures that can be dangerous, embarrassing, and severely restrict daily activities like driving, swimming, or employment. Beyond the seizures themselves, many individuals develop anxiety disorders about when the next seizure will occur, creating a vicious cycle.
The connection between stress, anxiety, and seizure threshold is well-established in both clinical observation and neuroscience research. Stress-induced cortisol release elevates neuronal excitability, effectively lowering the amount of electrical activity needed to trigger a seizure. Additionally, anxiety-related hyperventilation changes blood chemistry in ways that increase brain electrical instability, further lowering seizure threshold. During periods of high stress or anxiety, individuals with epilepsy often experience increased seizure frequency, suggesting that anxiety management is not just psychological support but functional seizure management. The amygdala's threat alarm directly influences seizure vulnerability.
Our technique restores parasympathetic nervous system activation and reduces chronic anxiety through targeted limbic recalibration. We lower the baseline threat-sensitivity that reduces seizure threshold, creating a neurophysiological environment less conducive to seizures. This isn't just stress management or relaxation counseling. It's targeted recalibration of the nervous system's electrical stability. You experience meaningful reductions in seizure frequency and increased predictability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Tics - Tourette Syndrome and Tic Disorders
This could be your breakthrough. Let's do this!
Your nervous system is firing unscheduled signals. It's time to redirect the neurological traffic. Tourette Syndrome and other tic disorders are neurodevelopmental conditions characterized by sudden, repetitive, nonrhythmic motor movements or vocalizations (tics) that are often experienced as irresistible and difficult or impossible to control. Tics can range from mild and barely noticeable to severe and highly disabling, significantly impacting social functioning and self-image, particularly in adolescence. Many individuals with tic disorders experience secondary anxiety and depression related to the social stigma and functional impairment caused by their tics.
The basal ganglia, a set of brain structures crucial for voluntary motor control and habit formation, plays a central role in tic expression and the anxiety-tic relationship. Anxiety triggers the basal ganglia and limbic system, causing a failure in inhibitory control that increases the frequency and severity of involuntary motor and vocal tics. Interestingly, anxiety about tics themselves becomes a key factor that worsens tics—stress about being watched or judged often intensifies tic expression, creating a feedback loop where anxiety amplifies the very symptoms individuals wish to control. The amygdala's hyperactivity disrupts the smooth regulation of the basal ganglia.
Our technique recalibrates the anxiety-basal-ganglia loop and restores smoother inhibitory control through targeted limbic intervention. We reduce the threat-state that amplifies tic frequency and dismantle the shame-surveillance cycle that keeps the nervous system braced against its own motor output. This isn't suppression training or forcing yourself to hide symptoms. It's recoding of the threat and motor circuits that keep tic expression intensified. You experience greater ease, reduced tic severity, and a nervous system that no longer escalates under observation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Functional Neurological Symptom Disorder - Motor and Sensory Symptoms
This could be your breakthrough. Let's do this!
Your nervous system is producing real neurological symptoms through dysfunctional signaling rather than structural destruction. Functional Neurological Symptom Disorder (FND), historically called conversion disorder, involves genuine disturbances in movement, sensation, speech, gait, coordination, vision, or other neurological functions that are not fully explained by a primary lesion, degenerative disease, or conventional structural finding. Symptoms can include weakness, tremor, abnormal gait, non-epileptic seizure-like episodes, sensory changes, speech blocks, facial asymmetry, or motor freezing. These symptoms are not faked, imagined, or voluntary. They are real outputs of a nervous system whose threat-processing, attention, prediction, and motor-control networks have become dysregulated.
The neurobiological mechanism involves disrupted communication between limbic threat circuits, salience networks, motor planning systems, and predictive coding pathways. The brain begins over-predicting danger, misallocating attention to bodily signals, and generating abnormal motor or sensory outputs that become self-reinforcing through hypervigilance, fear, and symptom-monitoring. Trauma, chronic anxiety, overwhelm, dissociation, or repeated stress can sensitize these networks so that normal movement or sensation becomes interrupted by threat-based neural interference. The symptom is functional, not fictional: the hardware may be intact, but the operating pattern is compromised.
Our technique targets the threat-signaling and predictive-control systems driving the symptom pattern. We reduce amygdala overactivation, recalibrate the salience network's fixation on symptom output, and restore smoother top-down and bottom-up communication between motor, sensory, and emotional systems. This is not telling you the symptom is all in your head. It's targeted recoding of the nervous system processes that are producing the symptom in real time. You regain trust in your body, reduced symptom volatility, and a brain that stops converting distress into neurological interference.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Psychogenic Movement Disorders - Stress Tics, Facial Guarding, and Functional Facial Motor Symptoms
This could be your breakthrough. Let's do this!
Your facial motor system may be acting like it is on threat duty even when no structural neurological damage is present. Psychogenic movement disorders are a functional sub-category of movement disorders in which psychological distress, chronic anxiety, or trauma dysregulation generates involuntary or semi-involuntary motor symptoms without the pattern being fully explained by a primary structural neurological disease. In this presentation, the symptoms center on facial and peri-ocular motor output: anxiety-driven facial tics or stress tics, psychogenic blepharospasm with involuntary eyelid squeezing or closure, stress blinking, grimacing, protective facial holding, and subtle but persistent facial asymmetries created by muscle guarding.
The neurobiological mechanism involves threat-state overactivation of the basal ganglia, limbic system, facial motor pathways, and habitual muscle-bracing networks. When the amygdala remains locked in vigilance, the face often becomes part of the defense system: the corrugator supercilii maintains a furrowed-brow alarm signal, the levator labii may hold a unilateral elevation that reads as a sneer or partial palsy, the orbicularis oculi can clamp into stress blinking or eyelid closure, and the small muscles of expression may remain chronically recruited as if the face must constantly monitor, mask, or defend. These are not imaginary symptoms. They are functional motor outputs shaped by anxiety, hypervigilance, affective masking, and semi-permanent guarding that can become self-reinforcing through shame and symptom-monitoring.
Our technique interrupts the distress-to-movement loop by recalibrating the threat circuitry driving the motor pattern. We reduce amygdala overactivation, dissolve the defensive reflex encoded into facial expression, and restore smoother signaling through the motor control systems so blinking, expression, and facial symmetry no longer get hijacked by protection strategies. This is not cosmetic coaching or endless behavior monitoring. It's targeted recoding of how your nervous system uses facial musculature and micro-expressions to broadcast danger. You regain relaxed symmetry, voluntary control, and a face that no longer feels conscripted into survival mode.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Parkinson's Disease - Freezing of Gait, Performance Fear & Movement Shutdown
This could be your breakthrough. Let's do this!
Your movement system may already be under strain, and anxiety can make it seize even harder. Parkinson's disease is a neurodegenerative movement disorder involving tremor, rigidity, slowed movement, gait disturbance, and progressive difficulty with automatic motor control. Many people with Parkinson's also experience freezing of gait, hesitation in doorways or crowded spaces, and abrupt motor shutdown that becomes dramatically worse under pressure, observation, startle, or fear of falling.
The neurobiological mechanism involves degeneration in basal ganglia circuits that normally smooth and automate movement, combined with limbic interference when the person becomes anxious. The amygdala and autonomic nervous system can hijack already fragile motor sequencing, causing feet to feel glued to the floor, stride length to collapse, and movement to become consciously effortful. Fear of freezing then becomes part of the freezing circuitry itself: the person scans for failure, anticipates embarrassment or falling, and the threat-state further jams motor execution.
Our technique targets the anxiety-motor interference layer by reducing amygdala activation, restoring calmer autonomic tone, and interrupting the fear-freezing feedback loop. This is not presented as a cure for Parkinson's disease or a replacement for neurology, medication, or rehabilitation. It is aimed at the stress-amplified component that makes gait, confidence, and movement reliability deteriorate further under threat. You experience reduced freezing reactivity, improved confidence in movement contexts, and a nervous system less likely to convert fear into motor shutdown.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Neurocardiogenic Syncope - Vasovagal Fainting, Startle Collapse & Fear-Based Blood Pressure Drop
This could be your breakthrough. Let's do this!
Your nervous system may be triggering a shutdown response when threat or overwhelm spikes too suddenly. Neurocardiogenic syncope, often overlapping with vasovagal fainting patterns, is the most common cause of fainting and involves abrupt drops in blood pressure and heart rate leading to dizziness, tunneling vision, nausea, heat, weakness, and loss of consciousness. Episodes are often triggered by fear, pain, needles, medical situations, prolonged standing, or emotional shock, leaving the person anxious about when the next collapse might happen.
The neurobiological mechanism involves dysregulated autonomic switching where the nervous system overcorrects under perceived threat. Instead of maintaining balanced arousal, the person flips into a parasympathetic crash that drains blood pressure and cerebral perfusion. The amygdala then encodes situations associated with prior fainting as danger contexts, meaning the anticipation of fainting becomes part of the fainting risk itself. This creates an elegant but destructive loop: fear of collapsing destabilizes the very physiology the person is trying to protect.
Our technique targets the fear-physiology loop by reducing amygdala reactivity to known triggers and recalibrating autonomic interpretation of bodily changes. This is not a substitute for cardiology, autonomic testing, hydration strategies, compression, or medical workup for fainting. It is aimed at the conditioned threat overlay that makes episodes more frequent, more anticipated, and more disabling. You experience reduced anticipatory panic, more stable response to known triggers, and a nervous system less likely to convert fear into shutdown.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Stiff Person Syndrome - Startle-Induced Rigidity, Spasm & Emotional Trigger Locking
This could be your breakthrough. Let's do this!
Your body may be treating sound, surprise, or emotion like a signal to lock down. Stiff Person Syndrome is a rare neurologic disorder involving progressive rigidity, painful muscle spasms, exaggerated startle, and severe sensitivity to sudden stimuli or emotional upset. Because attacks can be dramatic and disabling, the person often begins living in a state of constant anticipatory guarding, scanning for noises, interruptions, or emotional spikes that could trigger full-body spasm.
The neurobiological mechanism involves disordered inhibitory signaling in motor pathways, with startle and threat circuitry magnifying muscle rigidity when the nervous system is provoked. Emotional shock or fear can recruit the autonomic nervous system and make the body shift even faster into painful contraction. Over time, the amygdala learns that ordinary environments are full of possible spasm triggers, and the person becomes trapped in a loop where fear of the next spasm increases baseline muscular bracing and sensory reactivity.
Our technique addresses the fear-rigidity amplification loop, not the underlying rare neurologic disease process itself. It is not a replacement for neurology, immunotherapy, medication, mobility support, or specialist care. It targets the secondary threat-conditioning that causes the person's world to shrink around startle avoidance. You experience reduced anticipatory alarm, less emotional contribution to whole-body locking, and a nervous system that does not add unnecessary threat chemistry to an already vulnerable motor system.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Sleep, Somatic & Functional Disorders
Chronic Pain - Psychosomatic and Nervous System Amplification
This could be your breakthrough. Let's do this!
Your nervous system has trapped pain signals in an amplification loop. It's time to restore accurate pain signaling. Chronic pain that persists beyond reasonable healing timelines often involves nervous system amplification where the central nervous system produces pain signals that persist despite tissue healing, creating pain without ongoing injury. This creates a devastating trap: the nervous system remains in threat-based pain signaling, producing real pain that reinforces the perception of threat, which amplifies the pain signal. Beyond acute tissue damage, chronic pain is often sustained by anxiety, catastrophic thinking, movement avoidance, and nervous system trapped in a state of protective pain signaling.
The neurobiological mechanism involves central sensitization where the nervous system's pain-processing circuits become hyperactive and misaligned. Gate-control mechanisms that normally filter pain signals malfunction, allowing minor sensations to be interpreted as significant pain. When anxiety or threat-perception is present, the amygdala activates descending pain amplification pathways that literally amplify pain signal intensity at the spinal cord level. The insula becomes hyperresponsive to pain signals, the anterior cingulate cortex catastrophizes pain meaning, and the prefrontal cortex loses regulatory capacity. The nervous system becomes trapped in a state of self-perpetuating pain amplification.
Our technique recalibrates the pain-amplification circuitry by reducing threat perception and restoring accurate pain signal processing through targeted limbic intervention. We dissolve the anxiety-pain feedback loop and restore gate-control mechanisms. Pain signals normalize as the nervous system exits threat-based amplification mode. This isn't pain management or distraction. It's recoding of how your nervous system generates and sustains pain signals. You experience genuine pain reduction as the amplification system recalibrates.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
TMJ, Bruxism, Lockjaw, Jaw Clenching, and Masseter Tension
This could be your breakthrough. Let's do this!
Your jaw may be carrying more threat than your conscious mind can register. Temporomandibular dysfunction, bruxism, chronic jaw clenching, masseter tension, and stress-linked lockjaw patterns often emerge when the nervous system recruits the jaw as part of a chronic defense posture. This condition is specifically about jaw-centered symptoms: teeth grinding in sleep, daytime clenching you barely notice, jaw pain, temple pain, clicking or popping at the temporomandibular joint, limited opening, painful chewing, ear pressure, headaches, and a sense that the jaw is always braced for impact.
The neurobiological mechanism involves threat-state overactivation of trigeminal pain signaling, temporomandibular joint stress, and habitual muscle-armoring networks concentrated in the jaw. When the amygdala stays activated, the jaw becomes one of the body's preferred sites for storing defensive contraction. The masseter, temporalis, pterygoids, and surrounding fascial structures remain partially engaged, especially during sleep, high concentration, anger suppression, or hypervigilance. Over time, this bracing alters bite pressure, irritates the temporomandibular joint, amplifies pain through central sensitization, and teaches the nervous system to treat relaxation of the jaw as unsafe. Anxiety, trauma, and symptom-monitoring then reinforce the cycle.
Our technique targets the jaw-threat loop directly. We reduce amygdala-driven clenching, recalibrate the trigeminal and temporomandibular threat pathways, and restore a nervous system that no longer uses the jaw as a default armor plate. This is not just a mouth guard, stretching protocol, or reminder to unclench. It's targeted recoding of the chronic stress pattern driving jaw contraction, joint irritation, and pain amplification. You experience less grinding, easier opening, reduced jaw and temple pain, and a jaw that no longer feels locked into protective tension.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Insomnia and Sleep Hyperarousal
This could be your breakthrough. Let's do this!
Your nervous system learned to stay on alert at night when it should be resting. Sleep is where the threat-detection system downregulates. Insomnia is characterized by persistent difficulty initiating or maintaining sleep despite adequate opportunity, leading to daytime impairment. Insomnia is often perpetuated by sleep-related anxiety (anxiety about not sleeping), hyperarousal where the nervous system stays in alert/threat-detection mode throughout the night, racing thoughts about day stressors, and conditioned alertness where the bedroom becomes associated with worry-activation. Chronic insomnia profoundly impacts health, cognitive function, emotional regulation, and physical recovery.
The neurobiological mechanism involves failure of the parasympathetic nervous system to activate at night combined with amygdala hyperactivity that maintains threat-vigilance. The default mode network—which normally quiets during sleep—remains hyperactive. Hyperarousal involves elevated cortisol, norepinephrine, and other stress neurochemicals at night when they should be low. Worry-rumination activates prefrontal-limbic circuits, preventing the shift to sleep-mode. Sleep-related anxiety creates classical conditioning where the bed/bedroom becomes associated with threat-processing rather than rest. The nervous system becomes trapped in a state where threat-detection remains activated when nervous system resources should be devoted to repair and memory consolidation.
Our technique recalibrates night-time threat detection and restores parasympathetic activation through targeted limbic recalibration. We reduce sleep-related anxiety and reset the conditioned hyperarousal. Your nervous system regains capacity to shift into parasympathetic rest mode at night. This isn't sleep hygiene or stimulus control. It's recoding of how your nervous system manages threat-detection across the sleep-wake cycle. You experience restored capacity to sleep deeply, awakening refreshed.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Restless Legs Syndrome - Urge to Move, Night-Time Agitation & Sleep Disruption
This could be your breakthrough. Let's do this!
Your nervous system may be turning stillness into alarm. Restless Legs Syndrome (RLS) is characterized by an uncomfortable urge to move the legs, usually worsening during rest and in the evening, often described as crawling, buzzing, pulling, or electrical discomfort deep in the limbs. Many individuals with RLS experience anticipatory dread about bedtime, fragmented sleep, daytime fatigue, and escalating anxiety because quiet rest reliably becomes the moment symptoms intensify.
The neurobiological mechanism involves dysregulation across dopaminergic signaling, sensory processing, arousal systems, and sleep-wake control. Anxiety and hypervigilance increase the salience of internal limb sensations, while the amygdala and autonomic nervous system make the body treat stillness as if it were unsafe. The result is not simply movement for comfort but a learned nervous-system pattern where the absence of motion is experienced as mounting threat or agitation. Fear of symptoms then amplifies the symptoms themselves, especially at night.
Our technique targets the threat-coding that makes rest feel intolerable and recalibrates the nervous system's interpretation of internal leg sensations. This is not a substitute for iron workup, sleep medicine, or neurologic treatment where needed. It addresses the stress-reactive amplification, bedtime dread, and conditioned arousal loop that often hardens around RLS. You experience greater calm at rest, reduced fear of the evening window, and a nervous system more capable of tolerating stillness without escalating into motor urgency.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Narcolepsy Type 1 - Cataplexy, Sleep Attacks & Emotion-Triggered Shutdown
This could be your breakthrough. Let's do this!
Your sleep-wake boundary may be collapsing when the nervous system is hit by emotional intensity. Narcolepsy Type 1 is a neurologic sleep disorder characterized by overwhelming daytime sleepiness, sudden sleep attacks, fragmented night sleep, dream intrusion phenomena, and cataplexy, where strong emotions such as laughter, surprise, or fear trigger abrupt loss of muscle tone. Because the symptoms are dramatic and unpredictable, many individuals begin to fear emotion itself, public settings, or any circumstance where collapse or sudden sleep would be humiliating.
The neurobiological mechanism involves dysregulation of sleep-wake circuitry and orexin-hypocretin signaling, with limbic states often acting as trigger multipliers. Emotional spikes can destabilize already fragile muscle-tone and arousal control, while the amygdala's response to anticipation and embarrassment increases overall nervous-system volatility. The person becomes caught in a loop where fear of cataplexy or sleep attacks intensifies vigilance, fatigue, and symptom-monitoring, making the condition more functionally intrusive.
Our technique targets the anticipatory fear, shame, and trigger-reactivity that layer onto narcolepsy and make daily life narrower than the neurologic disorder alone would require. This is not framed as a replacement for sleep medicine, stimulant therapy, sodium oxybate, or neurologic care. It addresses the threat overlay that turns symptom possibility into chronic life-constriction. You experience reduced fear of symptom exposure, calmer response to emotional activation, and a nervous system less likely to amplify the disorder through constant anticipatory alarm.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Factitious Disorder - Medical Deception & Munchausen Syndrome
This could be your breakthrough. Let's do this!
Your nervous system learned that the only way to guarantee caring attention from others is through cultivating an identity as sick or vulnerable, and that fabricating or inducing illness is a rational strategy to secure the medical care, attention, and validation that you desperately need. Factitious Disorder (formerly known as Munchausen syndrome) is characterized by falsification of medical or psychological signs and symptoms, either by producing or exaggerating illness in oneself (Factitious Disorder Imposed on Self) or in another person, typically a dependent (Factitious Disorder Imposed on Another, previously called Munchausen by Proxy). The person deliberately produces false, misleading, or exaggerated symptoms, may engage in self-harm or refusal of appropriate medical treatment to maintain the sick identity, and pursues unnecessary medical procedures and investigations. Unlike malingering (where deception is for external gain like disability benefits), factitious disorder involves deception driven by psychological need—the person needs the sick identity for self-worth or relational purpose.
The neurobiological mechanism involves profound relational trauma history combined with dysregulation of the attachment and reward systems. The ventromedial prefrontal cortex encodes the sick/vulnerable identity as the only acceptable self and the only pathway to relational connection ("The only way people care about me is when I'm suffering"). The nucleus accumbens becomes dopamine-dependent on the specific rewards of sick-role attention: medical attention, healthcare provider focus, family mobilization, and the validation of suffering. The medial prefrontal cortex fails to maintain stable identity separate from the sick role—without the illness, the person experiences the terror of being nobody or unworthy. The anterior insula generates persistent bodily distress (learned hypochondriasis where normal sensations are interpreted as illness). The amygdala becomes hyperresponsive to abandonment threat and hyperactive in seeking reassurance. The orbitofrontal cortex has become locked into the calculation: "Illness = attention and care. Wellness = abandonment and rejection." For those who impose factitious illness on others (Munchausen by Proxy), additional pathology involves using another person's body to meet their own relational needs—the victim (usually a child) becomes an extension of the perpetrator's identity with no autonomy or bodily integrity.
Our technique addresses the profound relational trauma underlying the factitious behavior and rebuilds the ventromedial prefrontal cortex's capacity to maintain stable identity separate from illness or vulnerability. We recalibrate the nucleus accumbens to find genuine dopamine-reward in authentic relational connection, accomplishment, and valued contribution rather than in sick-role attention. We rebuild genuine capacity for relational vulnerability that doesn't require fabricated illness. We help the insula recalibrate health-anxiety and false bodily-threat interpretation. We address the amygdala's abandonment-terror through genuine relational repair. The person develops capacity for authentic identity and relational connection, freedom from the exhausting labor of maintaining false illness, genuine medical autonomy and bodily integrity, and the relief of being valued for your authentic self rather than for your suffering. For perpetrators of Munchausen by Proxy, recovery involves genuine recognition of the harm caused and development of capacity for appropriate boundaries and respect for others' bodily autonomy.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Anxiety Somatization & Health Anxiety - Anxiety Manifesting in Physical Symptoms
This could be your breakthrough. Let's do this!
Your nervous system learned that the primary location for expressing terror is your body. Anxiety doesn't stay in your mind—it floods into your gut, your heart, your head, creating physical symptoms that feel more real than the underlying anxiety. Anxiety somatization and health anxiety occur when anxiety manifests primarily through physical symptoms rather than cognitive/emotional symptoms. This includes anxiety-triggered gastrointestinal issues (IBS, functional dyspepsia, nausea, constipation, diarrhea), where the gut becomes the early-warning system for threat; and anxiety amplification of existing health conditions (diabetes, asthma, autoimmune disease, chronic pain), where normal disease symptoms trigger catastrophic anxiety that exceeds the condition's actual threat. In both cases, the insular cortex (interoceptive awareness) becomes hyperactive, transforming normal body-signals into perceived threats, creating feedback loops where physical symptoms trigger anxiety about physical symptoms.
The neurobiological mechanism involves the gut-brain axis bidirectional communication between amygdala/prefrontal cortex and the enteric nervous system via the vagus nerve. When the amygdala perceives threat, it triggers parasympathetic shutdown of digestion, causing the GI symptoms that then confirm the threat-perception. The insular cortex becomes hyperactive in perceiving both GI sensations and other physiological signals, amplifying normal body-function into perceived threat. The enteric nervous system becomes sensitized to anxiety cues and misinterprets normal GI activity as threat. The HPA axis activation releases cortisol which disrupts gut microbiota, GI motility, and intestinal permeability. In health condition contexts, the amygdala becomes hypersensitized to symptom-related threat perception, normal disease symptoms (blood sugar variation, occasional chest sensation, fatigue) trigger amygdala activation as if they signal acute emergency, the prefrontal cortex fails to appropriately contextualize disease symptoms, leading to catastrophic prognosis predictions, and compulsive health-checking temporarily reduces anxiety but negatively reinforces the threat perception.
Our technique recalibrates the insula's dysregulated interoceptive awareness and reduces the amygdala's threat perception of body sensations through targeted limbic intervention. We restore normal vagal tone and the gutbrain axis decoupling from threat-response. We help the amygdala distinguish between normal disease symptoms and actual acute threat. Your nervous system ceases amplifying normal body-signals into perceived emergencies. You experience restored capacity for GI function and normal digestion, acceptance of health conditions with proportional rather than catastrophic anxiety, freedom from health-checking compulsions and reassurance-seeking, and the experience of your body as capable rather than as a betrayer generating constant threat-signals.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Psoriasis - Stress-Reactive Neuroimmune Skin Flares
This could be your breakthrough. Let's do this!
Your skin may be expressing a nervous system that has learned to stay inflamed. Psoriasis is a chronic inflammatory skin condition involving red, scaly, painful, or itchy plaques that can flare unpredictably and create profound self-consciousness because the illness is visible to the outside world. While psoriasis has an immune and genetic basis, many individuals experience unmistakable worsening during periods of acute stress, shame, social conflict, sleep disruption, or chronic threat-state activation. The result is a skin condition that is both immunologic and neurologically amplified.
The neurobiological mechanism involves reciprocal signaling between the immune system, HPA axis, autonomic nervous system, and limbic threat circuitry. When the amygdala remains hyperactive, cortisol rhythm becomes dysregulated and inflammatory cascades become harder to resolve cleanly. The skin becomes a visible endpoint of neuroimmune signaling: itch, burning, plaque expansion, scratching, embarrassment, and social vigilance then feed further sympathetic activation. The person becomes trapped in a loop where stress worsens the flare and the flare becomes a chronic source of stress.
Our technique targets the stress-amplification layer of psoriasis by reducing limbic overactivation, restoring autonomic regulation, and interrupting the shame-inflammation feedback loop. This does not claim to replace dermatologic care, biologics, or medical management of autoimmune disease. It is targeted at the nervous-system contribution that makes flares more persistent, more reactive, and more distressing than they would otherwise be. You experience reduced stress-reactivity, less symptom amplification, and a body that is no longer treating every psychological strain as a signal to inflame the skin.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Misophonia
This could be your breakthrough. Let's do this!
Certain sounds trigger your amygdala's threat response as if they were survival dangers. Conscious transformation teaches your nervous system the difference. Misophonia, sometimes called 'Selective Sound Sensitivity Syndrome,' is a condition in which certain specific sounds (often called 'trigger sounds') provoke an intense, immediate emotional and physiological response ranging from intense disgust and anxiety to rage. Common trigger sounds include chewing, slurping, sniffling, or repetitive tapping. The response is involuntary and far more intense than would be considered proportionate, typically leading to avoidance of situations where these sounds occur and social isolation from family members and loved ones.
The neurobiological basis of misophonia involves an abnormally strong connection between the auditory cortex and the limbic system, particularly the amygdala and insula, which process emotional salience and feelings of disgust. A hyper-connection between the auditory cortex and the limbic system causes specific sounds to trigger an immediate, intense, and involuntary anxiety or rage response. The sound activates threat-detection faster than it can be processed cognitively, leading to automatic emotional reactions before conscious awareness is fully engaged. The auditory threat pathway has been overamplified.
Our technique dissolves the pathological auditory-limbic connection through targeted limbic recalibration while reducing overall threat-sensitivity. We recalibrate the specific auditory threat signals. Trigger sounds lose their power to provoke automatic emotional reactions. This isn't desensitization or acceptance therapy. It's swift recalibration of the auditory-limbic danger link. You notice trigger sounds without the overwhelming reactive response. Family dinners, social gatherings, and intimate relationships become accessible again.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Performance, Prosperity & Career
Burnout - Chronic Exhaustion and Depersonalization
This could be your breakthrough. Let's do this!
Your nervous system has been running in overdrive for so long that it lost the ability to shift gears. Burnout isn't laziness—it's a nervous system trapped in a state of chronic threat perception. Burnout is a state of emotional, physical, and mental exhaustion caused by prolonged exposure to stressors in work or caregiving contexts, characterized by emotional exhaustion, depersonalization (emotional distance, cynicism, reduced empathy), and reduced sense of accomplishment. Individuals with burnout experience profound fatigue despite rest, cynical disconnection from work and people, loss of meaning and purpose, physical illness, and sometimes complete incapacity to function. Burnout reflects a nervous system pathology, not personal weakness or moral failing.
The neurobiological mechanism involves chronic activation of the stress response system that eventually leads to depletion of neurotransmitters (serotonin, dopamine, norepinephrine, cortisol dysregulation) and exhaustion of the hypothalamic-pituitary-adrenal axis. Prolonged threat-state consumes neural resources devoted to repair, memory consolidation, and meaning-making. Depersonalization emerges as a protective dissociation when the nervous system can no longer sustain emotional engagement. The prefrontal cortex becomes progressively compromised, reducing executive capacity and emotional regulation. The brain enters a state of 'learned shutdown' where further effort is perceived as dangerous. The default mode network becomes dysregulated, leading to loss of meaning and purpose.
Our technique recalibrates the nervous system from chronic threat-state through targeted limbic recalibration and restoration of meaning-systems. We restore the capacity to downregulate threat-perception and re-engage the parasympathetic nervous system. Your nervous system regains capacity for genuine rest, renewed energy, and restored sense of purpose. This isn't vacation or work-life balance advice. It's recoding of how your nervous system responds to occupational stress. You experience restoration of vitality, genuine emotional connection, and renewed capability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Hyper Cynicism - Depressive Realism, Pervasive Distrust & Defensive Negativity
This could be your breakthrough. Let's do this!
Your nervous system may have decided that hope is what gets people hurt. Hyper cynicism is not ordinary skepticism or healthy discernment. It is a rigid, overlearned interpretive stance in which the mind narrates people, systems, motives, and future outcomes through a lens of betrayal, futility, corruption, or inevitable disappointment. The person may feel that they are simply being "realistic" while everyone else is naive, sentimental, or self-deceived. In some individuals this resembles what has been called depressive realism: a stark, linear, bias-stripped view of life in which optimism feels dishonest and cynicism feels like truth. In more severe or personality-structured forms it can overlap with pervasive distrust, including paranoid predictions of betrayal or harm, or schizoid-style detachment where cynicism functions as a defensive wall against the vulnerability of social connection. This stance is often a compensation for the opposite pole: when defensive idealization, wish-based thinking, or naive trust has previously exposed the person to humiliation, exploitation, betrayal, or moral injury, the mind may swing into hyper cynicism to make sure openness never becomes that dangerous again. In workplace variants, the same stance gets projected onto employers, leadership, missions, customers, or the entire concept of meaningful work, especially after chronic overextension, hypocrisy exposure, or repeated exploitation. In relationship variants, the nervous system may begin treating intimacy itself as a setup for disappointment, using sarcasm, suspicion, emotional distance, or preemptive contempt to avoid dependence, grief, or humiliation. It is also common in occupational burnout, where chronic overtaxing leads to emotional distance, negativism, and contempt for the entire work system, and in moral injury, where the person begins to interpret future people and institutions through a hardened lens designed to prevent ever being fooled or violated again.
The neurobiological mechanism involves chronic threat-based prediction dominating interpretation. The amygdala and salience systems bias attention toward evidence of danger, hypocrisy, incompetence, betrayal, or collapse. The anterior cingulate cortex remains over-engaged in error-detection and contradiction-monitoring, constantly scanning for what is wrong or unsafe. The ventromedial prefrontal cortex develops hardened beliefs such as "people always disappoint," "systems are rigged," "every relationship ends in betrayal," or "hope is for fools," and then uses those beliefs to interpret new information before it is fully evaluated. The dorsolateral prefrontal cortex may construct elaborate justifications for the cynical stance, making it feel intellectually superior rather than emotionally defended. The insula tags interpersonal contact, institutions, work obligations, and future-oriented thinking with disgust, dread, or deadness rather than curiosity or possibility. In many cases this is a compensatory correction against a prior history of overtrust, idealization, or denial: the nervous system learns that if it expects the worst, it cannot be fooled in the same way again. In burnout, the PFC narrates chronic limbic exhaustion as the uselessness of the work, the mission, or the people involved. In relationship-focused variants, attachment cues themselves become fused with anticipated disappointment, engulfment, betrayal, or ridicule, so distance starts feeling safer than tenderness. In moral injury, future trust is filtered through the memory of value-violation so the organism is never caught undefended again. What looks like philosophical realism is often a nervous system that no longer feels safe enough to generate openness, trust, or adaptive optimism.
Our technique targets the threat-prediction machinery beneath the cynical narrative. We recalibrate the amygdala's reflexive expectation of betrayal, restore flexibility to the ventromedial prefrontal cortex's world-models, and reduce the anterior cingulate's compulsive fixation on what's wrong, corrupt, or doomed. We help the insula distinguish true danger from habituated negativism and re-open access to social, relational, vocational, and existential engagement without forcing fake positivity. This is not an attempt to make someone gullible, compliant, or blind to genuine corruption. It is the restoration of discernment without totalized distrust. You experience less compulsive negativism, reduced need to protect yourself through contempt or emotional distance, greater capacity to evaluate people, work systems, and intimate relationships realistically without collapsing into bitterness, and a nervous system that no longer mistakes openness for danger or cynicism for truth itself.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Defensive Idealization - Unrealistic Optimism, Reality Avoidance & Wish-Based Thinking
This could be your breakthrough. Let's do this!
Your nervous system may have decided that the only tolerable future is the one it beautifies, sanitizes, or spiritually guarantees. Defensive idealization is the opposite pole of hyper cynicism. Instead of anticipating betrayal, collapse, or disappointment, the mind overcorrects toward unrealistic optimism, selective attention to reassuring signs, and a refusal to metabolize contradictory evidence. This is not grounded hope, resilience, or mature faith. It is an overlearned protective style in which danger gets minimized, motives get idealized, and complexity gets replaced with certainty that "everything will work out" if one just stays positive, trusts hard enough, or refuses to look directly at what is happening. In some individuals it appears as chronic denial, in others as relational idealization, redemptive certainty, suggestibility to charismatic personalities, or wish-based thinking that treats desire as evidence. This stance is often a compensation for the opposite pole: when hyper cynicism, chronic distrust, or repeated anticipation of betrayal has become unbearable, the mind may swing toward idealization, magical reassurance, and naive faith because certainty feels safer than living in permanent suspicion. This can create unusual vulnerability to narcissists, conmen, manipulative gurus, apocalyptic belief systems, superstition, and rigid religiosity, because the person's need for reassurance outruns their reality-testing. In more spiritualized forms it can resemble spiritual bypassing, where grief, anger, accountability, and skepticism are skipped in favor of destiny narratives, miraculous explanations, prophetic certainty, or the conviction that discernment itself is a lower form of consciousness.
The neurobiological mechanism involves top-down inhibition of threat information rather than healthy integration of it. The ventromedial prefrontal cortex generates overly coherent positive narratives that suppress disconfirming evidence before it can fully update the model of reality. The anterior cingulate cortex becomes less willing to sustain contradiction, ambiguity, or error-signals, so the person exits uncertainty too quickly and lands in premature reassurance. The dorsolateral prefrontal cortex may become recruited into rationalization, constructing polished explanations for why obvious risks do not apply, why boundaries are unnecessary, why a charismatic person must be trustworthy, or why improbable claims should be accepted because they feel meaningful. The amygdala's warnings may be chronically bypassed, numbed, or reinterpreted as mere negativity rather than useful data. The insula's uncomfortable signals of dread, aversion, or intuition are overruled by a learned mandate to stay uplifted, surrendered, faithful, or certain. In many cases this is a compensatory correction against a prior state of bitterness, suspicion, or collapse into distrust: the nervous system reaches for idealization because unbuffered cynicism feels intolerable. In relationship variants, it can appear as idealizing unavailable, exploitative, or grandiose partners, dismissing red flags as tests of love or faith, and repeatedly converting manipulation into a redemption story. In spiritual or superstitious variants, coincidence gets over-read as destiny, authority gets confused with wisdom, and the need for cosmic safety can override evidence, boundaries, and independent judgment. What looks like positivity is often a nervous system that cannot yet tolerate grief, disillusionment, uncertainty, or the pain of seeing clearly.
Our technique restores contact with reality without collapsing the person into despair or cynicism. We help the nervous system tolerate ambiguity, loss, and contradiction so optimism no longer has to be inflated into denial. We recalibrate the ventromedial prefrontal cortex's need for redemptive certainty, strengthen the anterior cingulate's capacity to stay with disconfirming evidence, and restore the insula's role as a source of valid internal warning rather than something to override with affirmations, prophecy, or charm. This is not an attack on hope, meaning, spirituality, or genuine faith. It is the restoration of grounded hope that can face facts. You experience less compulsive idealization, reduced susceptibility to manipulators and grandiose personalities, greater ability to distinguish trust from fantasy and reverence from submission, clearer perception of red flags without collapsing into paranoia, and a nervous system that no longer mistakes denial for faith or wish-based thinking for wisdom.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Perfectionism - Impossible Standards and Self-Imposed Threat
This could be your breakthrough. Let's do this!
Your nervous system adopted an impossible standard and now treats anything short of perfection as threat. It's time to recalibrate what 'good enough' actually is. Perfectionism is characterized by setting impossibly high standards, persistent self-criticism for minor imperfections, and anxiety about making mistakes or being less than excellent in any endeavor. Individuals with perfectionism experience chronic stress, procrastination (avoiding tasks where perfectionism makes completion impossible), anxiety, depression, and often underperformance ironically because perfectionism becomes paralyzing. Perfectionism shares more neurobiological features with anxiety disorders than with goal-setting or excellence-seeking. The standards are self-imposed threats, not adaptive goals.
The neurobiological mechanism involves amygdala-driven threat-perception in response to imperfection or mistakes, combined with a perfectionist's hyperactive anterior cingulate cortex that generates persistent error-detection and self-criticism. The amygdala treats making mistakes or producing imperfect work as social threat or competence threat, triggering anxiety. This drives compulsive checking, revision, and reassurance-seeking. Procrastination emerges not from laziness but from anxiety: the nervous system avoids initiating tasks where perfectionism standards create threat-perception. The perfectionist becomes trapped in a state where performance-initiation generates anxiety, prevention generates guilt, and the standards themselves become a source of chronic threat.
Our technique recalibrates the threat-perception in response to imperfection and reduces the amygdala's sensitivity to minor mistakes through targeted limbic intervention. We restore accurate threat/non-threat assessment where true excellence becomes achievable without perfectionism-based anxiety. Your nervous system distinguishes between genuine quality and perfectionist threat-magnification. This isn't self-compassion training or standards reduction. It's recoding of how your nervous system encodes mistakes and imperfection as threat. You access genuine excellence production without the perfectionism-based anxiety and paralysis.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Test Anxiety
This could be your breakthrough. Let's do this!
High-stakes performance paralyzes your nervous system despite knowing the material. Your brain learned that tests equal threat. Test anxiety is a specific performance anxiety manifesting during high-stakes academic testing where despite adequate preparation and knowledge, individuals experience debilitating anxiety that blocks access to knowledge and interferes with performance. Individuals with test anxiety experience racing thoughts, 'brain freeze,' physical panic symptoms, catastrophic predictions of failure, and significant score decrements despite genuine understanding of material. This creates a vicious cycle where poor performance due to anxiety then generates prognosticating anxiety about future tests. Test anxiety can severely impact educational trajectories and long-term academic achievement.
The neurobiological mechanism involves amygdala hijack triggered by evaluation threat that blocks access to knowledge stored in hippocampus and cortex. When the amygdala perceives high-stakes threat, prefrontal cortex suppression occurs, limiting working memory and executive function access. The stress neurochemical cascade further impairs prefrontal function. Performance decrements due to anxiety then become encoded as predictors that 'tests are dangerous situations where performance fails,' further conditioning amygdala reactivity to testing contexts. The nervous system learns to treat test-taking as a threat to status and competence, triggering protective mechanisms that ironically prevent successful performance.
Our technique recalibrates the evaluation-threat perception in testing contexts through targeted limbic intervention. We dissolve the amygdala hijack during high-stakes academic performance and restore executive function and knowledge access. Your brain regains ability to access learned knowledge under test conditions. This isn't test-prep or anxiety management techniques. It's recoding of how your nervous system responds to academic evaluation threat. You experience genuine calm during testing with full access to knowledge and capability.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Glossophobia - Fear of Public Speaking
This could be your breakthrough. Let's do this!
Your brain perceives an audience as a firing squad. It's time to reclassify what witnessing actually means. Glossophobia, the fear of public speaking, is one of the most common specific phobias and social anxieties in the general population. Individuals with glossophobia experience intense anxiety, physical symptoms like trembling and accelerated heart rate, and often engage in significant avoidance of public speaking situations. This phobia can substantially limit career advancement, educational opportunities, and social participation, as public speaking is ubiquitous in professional and academic life.
The neurobiological mechanism involves heightened amygdala reactivity to social evaluation threat combined with anterior insula activation related to bodily awareness. The prospect of being judged by an audience activates the limbic threat-detection system, triggering sympathetic nervous system activation that causes physical symptoms like trembling, sweating, and racing heart—symptoms that the individual then becomes hypervigilant to, creating a feedback loop of escalating anxiety. The social threat becomes compounded by interoceptive threat (fear of one's own anxiety symptoms).
Our technique recodes the amygdala's threat coding for audiences through targeted creative intervention. We dissolve the social-evaluation threat hijack and replace it with genuine access to your authentic voice and message. Audiences transform from 'judges' to 'witnesses' in your mind's threat assessment. Physical anxiety symptoms evaporate as the threat signature recalibrates. This isn't confidence-building or gradual practice. It's swift recoding at the neurological level. Powerful public speaking competence emerges within sessions.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Performance Anxiety - Generalized Evaluation Anxiety
This could be your breakthrough. Let's do this!
Your amygdala perceives being watched or judged as social death. It's time to recalibrate that threat signal. Performance anxiety, beyond specific contexts like public speaking, is a pervasive anxiety about being evaluated, judged, or observed in any situation where performance or competence will be assessed. Individuals with generalized performance anxiety experience trembling, sweating, racing thoughts, and panic whenever their actions, knowledge, or abilities might be scrutinized—during meetings, presentations, tests, interviews, or even casual conversations with authority figures. This anxiety can severely restrict career advancement, educational achievement, and social participation.
The neurobiological mechanism involves amygdala hyperactivity in response to evaluation-threat combined with prefrontal cortex suppression. When the nervous system perceives potential judgment, the amygdala interprets this as social threat to status and belonging. This triggers sympathetic activation (visible physical symptoms) and suppression of executive function (creating the paradoxical performance decrements that the individual fears). The insula becomes hyperactive, amplifying awareness of physical symptoms, which further amplifies anxiety in a feedback loop. Social evaluation literally activates the same threat response as physical danger.
Our technique recalibrates the social-evaluation threat response through targeted limbic intervention. We dissolve the automatic amygdala hijack in response to evaluation and restore executive function under performance pressure. Trembling, sweating, and racing thoughts subside as the threat signal resets. This isn't confidence building or gradual exposure. It's recoding of how your nervous system interprets social evaluation. You access genuine calm and cognitive clarity in performance situations, with your actual capabilities accessible regardless of observation or judgment.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Stage Fright - Live Performance Anxiety & Audience-Triggered Freeze Response
This could be your breakthrough. Let's do this!
Your nervous system perceives an audience watching you perform as an acute existential threat—your body floods with fight/flight/freeze activation, your voice trembles, your limbs become rigid, and you lose access to the abilities you have in private. Stage fright is a specific manifestation of performance anxiety characterized by acute sympathetic nervous system activation triggered specifically by the presence of a live audience or the knowledge that you're being watched during performance. Unlike general anxiety or social anxiety, stage fright is tightly bound to the act of performing—singing, speaking, dancing, acting, playing an instrument, presenting. The individual may be entirely capable, confident, and articulate in rehearsal or conversation, but the moment they step on stage or face the prospect of live performance, their nervous system perceives a survival threat and activates freeze, tremor, voice constriction, memory loss, or dissociation. Common presentations include vocal tremor or squeaking, memory blanks despite knowing material thoroughly, rigid posture or movement, accelerated heartbeat, nausea, dry mouth, difficulty breathing, tunnel vision, and a sense of unreality or watching oneself from outside the body.
The neurobiological mechanism involves hyperactivation of the amygdala in response to the neurologically primitive threat-signal of "being watched by an audience"—humans have ancient nervous system programming that interprets being visually focused on by multiple eyes as a predation threat or a status-threat. The amygdala's threat-detection triggers a cascade: the sympathetic nervous system floods the system with adrenaline and cortisol, the anterior cingulate cortex (executive function and attention regulation) becomes hypoactive, the medial prefrontal cortex (social self-consciousness and self-representation) becomes hyperactive creating acute self-awareness and self-scrutiny, and the dorsal anterior insula becomes hyperactive generating acute interoceptive fear (you become hyperaware of your own body sensations, racing heart, shaking, which further triggers threat-response). The brainstem's locus coeruleus (arousal center) fires intensely, creating hypervigilance and redirecting all cognitive resources toward threat-detection and survival-response rather than toward the performance task itself. The motor cortex becomes dysregulated—fine motor control is suppressed in favor of gross motor threat-responses (fighting or fleeing show up as tremor, rigidity, or uncontrolled movement), and learned motor sequences (the muscle memory of playing an instrument, choreography, or speaking patterns) become inaccessible because the nervous system has abandoned learned behavior in favor of primitive survival scripts. The posterior inferior parietal cortex (sense of body ownership and embodiment) becomes dysregulated, creating the sensation of being outside your body or watching yourself perform from a distance. The Wernicke's area (language production) often becomes hypoactive, creating vocal constriction, voice loss, or the sensation that the words won't come out. Often, past experiences of performance failure, humiliation, criticism by authority figures during childhood, or public embarrassment have created deep threat-associations with being visually focused on and evaluated. Additionally, perfectionism and early messages that "being watched means being judged" create additional layers of threat-encoding.
Our technique dissolves the amygdala's threat-encoding by directly neutralizing the primitive "being watched means danger" association at the neurochemical and neural circuit level. We reprogram the threat-signal itself so the presence of an audience no longer triggers the cascade of sympathetic activation. We strengthen the medial prefrontal cortex's stable self-representation independent of external observation—your worth and performance quality are not determined by being watched. We restore dorsal anterior insula regulation so body sensations (heartbeat, breathing) register as normal arousal rather than threat. We restore the anterior cingulate and dorsolateral prefrontal cortex so executive function and genuine attention to the performance task automatically override threat-scanning. We help the motor cortex and cerebellum restore full access to learned motor sequences by recalibrating the nervous system's behavioral-availability hierarchy. We address traumas and early experiences that encoded watching-by-others as dangerous, neutralizing those threat-memories at source. You experience swift elimination of sympathetic flooding during performance, immediate restoration of access to your full abilities and learned skills, fluid vocal quality and movement, sharp memory access and executive function, genuine freedom and enjoyment during performance, and the capacity to take authentic artistic risks without the nervous system overriding your performance.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.General Performance Issues
This could be your breakthrough. Let's do this!
You know what to do, but when it matters, your nervous system hijacks your capability. Performance becomes blocked by threat-detection about the performance itself. Performance issues encompass situations where individuals can execute skills in low-stakes contexts but experience dysfunction when performance has perceived consequences (evaluation, competition, stakes, audience, time pressure). Whether academic, athletic, artistic, professional, or social performance, the nervous system perceives the performance context as threat and triggers the freezing, hyperarousal, or cognitive disruption that prevents effective performance.
The neurobiological mechanism involves the amygdala perceiving performance contexts as social threat where evaluation and judgment threaten status and worth. The prefrontal cortex becomes suppressed as amygdala activation increases, leading to working memory shutdown and access to learned skills becomes blocked. Stress neurochemicals (adrenaline, cortisol) increase in a way that impairs executive function and fine motor control despite enhancing gross motor activation. The anterior cingulate cortex may generate error-detection hyperactivity, making the nervous system hypercritical of performance in real-time, creating performance disruption through internal commentary.
Our technique recalibrates the amygdala's threat perception of performance contexts through targeted limbic intervention. We restore executive function and skill access when performance stakes are present. Your nervous system ceases treating performance as social threat and maintains prefrontal regulation. You experience genuine performance capability when stakes are present and freedom to execute skill at full capacity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Chronic Procrastination, Failure to Launch & Incompletions - Executive Dysfunction & Aversion-Based Avoidance
This could be your breakthrough. Let's do this!
Your nervous system has learned that starting, sustaining focus on, or completing important tasks generates intolerable dysphoria—shame, anxiety, self-doubt—so it reflexively triggers avoidance even when the task is crucial for your life trajectory. Chronic procrastination and failure to launch encompasses a pervasive pattern of task initiation failure, sustained focus collapse, or inability to cross the finish line on important projects—despite the individual often being highly capable and intelligent. Unlike occasional procrastination, this pattern is neurologically driven: the person wants to begin the task, may have perfect competence to execute it, but when the moment arrives to start or push through, the nervous system triggers aversion-cascade that makes the task feel overwhelmingly dysphoric, impossible, or dangerous. The result is systematic incompletions—projects left at 95%, applications never submitted, jobs never started, degrees never finished, creative work never completed. The individual often experiences profound shame, self-judgment, identity as "lazy" or "broken," and escalating life consequences: missed opportunities, derailed careers, lost relationships, financial crises. The paradox is the intelligence and often extreme capability coexisting with systematic inability to activate.
The neurobiological mechanism involves dysregulation of the ventromedial prefrontal cortex's reward-prediction for future outcomes combined with hyperactive amygdala threat-response specifically to task initiation and sustained focus. When the person approaches a significant task, the amygdala fires with threat-intensity—the task triggers deep associations: failure-shame, judgment, exposure of inadequacy, loss of autonomy, or drowning in overwhelm. The ventromedial prefrontal cortex, which normally generates motivation by computing the value of delayed rewards ("if I complete this, I'll achieve X"), fails to generate sufficient dopamine-responsive motivation—the future reward feels distant and uncertain while the present dysphoria of starting is immediate and intolerable. The anterior cingulate cortex, which monitors for conflict and generates "push through" signals, becomes dysregulated—instead of amplifying effort-allocation when difficulty is encountered, it amplifies threat-perception. The dorsolateral prefrontal cortex (sustained focus and working memory) becomes hypoactive—when the person tries to maintain focus, the nervous system's resources are redirected to threat-response rather than task-execution. The midbrain's dopamine systems show dysregulated delay-discounting: present aversion is neurochemically weighted far more heavily than future reward, creating the sensation that the pain of starting is infinitely large compared to the benefit of completion. The nucleus accumbens becomes dopamine-dependent on avoidance behaviors (scrolling, distraction, escape activities) which provide immediate relief, reinforcing the procrastination loop. Often, childhood experiences of harsh criticism for mistakes, perfectionist standards creating terror of inadequacy, early failure-shaming, or developmental experiences where admitting incompetence resulted in punishment or abandonment have created deep threat-encoding around task performance and evaluation. Additionally, ADHD, anxiety, or depression frequently co-occur and compound the pattern. The person may have lost jobs, relationships, educational opportunities, or creative identity due to the procrastination-incompletions pattern, which then creates meta-shame ("I'm someone who can't follow through") that further increases task-aversion.
Our technique eliminates the amygdala's threat-encoding around task initiation and completion by directly neutralizing the false associations between challenging work and existential danger. We restore dopamine responsiveness to the completion of even small task increments—rewiring the nucleus accumbens so genuine task-progress becomes neurochemically reinforcing rather than avoidance-behaviors. We recalibrate the ventromedial prefrontal cortex's value-computation for delayed rewards so future outcomes feel genuinely motivating in real-time. We strengthen the anterior cingulate and dorsolateral prefrontal cortex's capacity to sustain focus and override threat-signals when difficulty emerges. We dissolve the shame-narratives and perfectionism-encoding that made task-initiation feel like existential risk. We address any underlying ADHD, anxiety, or trauma that exacerbates the pattern. We recondition the nervous system so the act of starting and sustaining focus on meaningful work generates genuine interest and activation rather than aversion-cascade. You experience immediate elimination of procrastination-driven dysphoria, swift task initiation and completion capacity, restoration of genuine motivation and interest in meaningful work, freedom from shame-cycles, recovery of creative and professional identity, and the systematic capacity to follow through on important life projects.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.AI Anxiety and Technophobia - Fear of Artificial Intelligence
This could be your breakthrough. Let's do this!
Your nervous system perceives AI and technological change as existential threat. It's time to recalibrate threat-assessment in an age of technological transformation. AI anxiety is a form of specific anxiety about artificial intelligence, autonomous systems, technological automation, or technological disruption characterized by fear of AI replacing human capability, loss of employment/relevance, loss of control to machines, or existential risk from superintelligence. Individuals with AI anxiety experience persistent worry about technological job displacement, anxiety about AI making autonomous decisions affecting their lives, fear about loss of human agency, and generalized technophobia that creates avoidance of new technologies. This anxiety is becoming increasingly prevalent as AI capabilities advance and societal uncertainty about AI implications persists.
The neurobiological mechanism involves uncertainty-based amygdala activation combined with realistic concern about technological disruption. The amygdala becomes hyperreactive to information about AI advancements, job displacement reports, or AI capability expansions—interpreted as existential threat. The loss of control element triggers heightened amygdala activation: when humans cannot predict or control AI system behavior, the nervous system perceives this as threat. Media narratives about AI risk and job displacement amplify this perception. For individuals with preexisting anxiety or perfectionism, AI uncertainty becomes encoded as catastrophic threat. The nervous system remains in a state of vigilance to AI-related threat cues.
Our technique recalibrates threat-perception in response to AI and technological change through targeted limbic intervention. We restore accurate threat-assessment: distinguishing between genuine risks requiring adequate attention and anxiety-amplified catastrophic projections. Your nervous system regains capacity to engage with new technologies without threat-hijacking. This isn't technology education or exposure therapy. It's recoding of how your nervous system processes uncertainty about AI and technological change. You experience genuine curiosity and adaptive concern without the anxiety-based avoidance and rumination.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.General Financial Anxiety & Cynicism
This could be your breakthrough. Let's do this!
Your nervous system learned that money represents fundamental threat—scarcity, powerlessness, or existential insecurity—and now generates chronic anxiety and cynical beliefs about financial systems, fairness, and your own financial capacity. General financial anxiety is characterized by persistent, pervasive worry about money, financial decisions, and financial security regardless of objective financial status. The person may experience chronic money-worry despite adequate or abundant resources (generalizing past scarcity to present reality), feel trapped by perceived unfair financial systems, develop cynical beliefs that "the game is rigged" or "financial success is impossible for me," and experience decision-paralysis about financial matters due to fear of catastrophic mistakes. This differs from specific phobias (chrometophobia) or trauma responses (financial flashpoint trauma)—it is chronic background anxiety that colors all financial perception.
The neurobiological mechanism involves dysregulation of threat-assessment systems applied to financial domain, combined with attentional bias toward financial threat-information and learned helplessness from past scarcity. The amygdala remains subclinically active to financial stimuli even in safe financial conditions, producing persistent low-grade anxiety. The anterior cingulate cortex (threat monitoring) generates excessive focus on potential financial problems or mistakes. The ventromedial prefrontal cortex has encoded beliefs about financial unfairness or impossibility based on past experience (family scarcity, poverty, financial instability) and fails to update those beliefs based on current objective evidence. The dorsolateral prefrontal cortex's executive function becomes suppressed under financial anxiety, producing money-related procrastination and decision avoidance. The insula generates persistent bodily sensations of financial threat—tension, dread, or dysphoria when handling money or reviewing finances. The anterior insula may encode cynical interpretations of financial information ("the system is rigged," "I'm incapable")—essentially a learned cynicism that becomes self-perpetuating.
Our technique recalibrates the threat-assessment systems specifically for financial stimuli, dissolving the amygdala's threat-encoding of money and financial decisions. We reprogram the ventromedial prefrontal cortex's beliefs about financial fairness and personal capacity, replacing cynicism with realistic appraisal. We restore the dorsolateral prefrontal cortex's executive function so financial decisions become possible. We recalibrate the anterior insula's cynical interpretations and replace them with discernment (genuine danger vs. normal financial uncertainty). We eliminate the attentional bias toward financial threat-information. You experience profound reduction in chronic money-worry, restoration of financial decision-making capacity, elimination of money-related decision paralysis, replacement of cynicism with realistic financial assessment, ability to engage with finances without anhedonia or dread, and a nervous system that differentiates actual financial threat from normal financial uncertainty.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Scarcity Mindset - Chronic Resource Poverty & Survival-Mode Fixation
This could be your breakthrough. Let's do this!
Your nervous system remains locked in a survival-mode algorithm designed for genuine deprivation, and now that algorithm runs continuously even when resources are available. Scarcity mindset is a psychological state resulting from perceived or actual lack of resources (time, money, food, safety) that creates a tunnel-vision effect where an individual focuses entirely on immediate needs and survival, at the expense of long-term planning and well-being. The person in scarcity mindset experiences intensified stress, reduced cognitive capacity for complex decisions, compulsive behaviors around resource acquisition, and a neurological inability to consider long-term consequences. Even when objective resources become available, the nervous system continues operating in scarcity-mode, leading to poor financial decisions, inability to save, hoarding behaviors, and chronic stress. This is closely tied to fear of homelessness and survival-threat anxiety, where the brain maintains constant high cortisol stress response due to perceived existential danger.
The neurobiological mechanism involves chronic activation of the HPA axis (hypothalamic-pituitary-adrenal) in response to perceived resource insufficiency, creating persistent elevation of cortisol and adrenaline. The amygdala remains in hypervigilant threat-scanning, constantly monitoring for resource-threat. The ventromedial prefrontal cortex's future-planning and delayed-gratification capacity becomes suppressed by the dominance of amygdala threat-response—the nervous system computes that it must prioritize immediate survival over future outcomes. The dorsolateral prefrontal cortex shows reduced capacity for complex planning and abstract thinking as cognitive resources are redirected toward survival-mode processing. The insula becomes hypersensitive to internal distress signals, creating the sensation of urgency and deprivation even when resources are objectively secure. The nucleus accumbens becomes dysregulated—it fails to generate reward from healthy long-term goals and instead becomes responsive only to immediate resource-acquisition. Often, genuine childhood deprivation, early scarcity experiences, or parents with scarcity-mindset have encoded the nervous system's baseline as "resources are never enough." Even when the person achieves financial security, their nervous system's threat-baseline remains calibrated to scarcity, creating the paradox of financial sufficiency coexisting with felt deprivation.
Our technique recalibrates the HPA axis's threat-assessment and the amygdala's resource-threat hypervigilance. We help the ventromedial and dorsolateral prefrontal cortex recover capacity for long-term planning and future-reward computation. We reprogram the insula's distress-sensitivity so the person's internal signal of safety matches their actual resource-reality. We address any early deprivation trauma that established the scarcity-baseline and reprogram those neural encodings. We help the nucleus accumbens discover genuine dopamine-reward in long-term security-building rather than only in immediate consumption. We dissolve the fear-of-homelessness threat-encoding and help the person's nervous system recalibrate to accurate threat-assessment. You experience dramatic reduction in survival-mode activation despite objective security, restored capacity for long-term planning and delayed gratification, reduction in chronic stress and cortisol-elevation, ability to build and maintain financial security without neurological sabotage, and genuine internal experience of sufficiency and safety.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Money Dysmorphia - Distorted Financial Self-Perception & Wealth Misalignment
This could be your breakthrough. Let's do this!
Your mirror for financial reality is broken—you see yourself as desperately poor while sitting on savings, or you spend lavishly while drowning in debt, unable to reconcile the gap between your financial reality and your internal felt sense of your wealth. Money dysmorphia occurs when an individual has a fundamentally distorted perception of their actual financial standing, creating persistent misalignment between objective financial reality and internal felt experience of wealth or poverty. This can manifest as: (1) feeling poor or financially insecure despite having significant savings or income; (2) spending lavishly or taking financial risks despite being in deep debt, maintaining the image of wealth while the reality deteriorates; (3) inability to accurately track or understand one's actual financial position; or (4) intense shame or unworthiness despite financial success. The individual's spending behaviors, financial decisions, and emotional responses are driven by internal felt sense rather than reality, often creating self-fulfilling prophecies where distorted perception eventually generates matching financial consequences.
The neurobiological mechanism involves dysregulation of the anterior insula (perception of internal financial status) combined with dissociation between objective financial data and the ventromedial prefrontal cortex's self-worth computation. The person's interoceptive system generates a persistent signal of financial inadequacy or shame regardless of objective financial markers. The medial prefrontal cortex encodes net worth with self-worth—if the felt sense is "I'm worth less than I claim," the person unconsciously generates spending or financial sabotage that aligns actual financial status with internal self-worth narrative. The ventromedial prefrontal cortex fails to update its financial threat-assessment even when presented with objective evidence (bank statements, asset lists, income documentation). The nucleus accumbens shows dysregulated reward-response—either it generates dopamine-reward from image-maintenance spending despite financial danger, or it fails to generate any reward from actual financial security if the internal narrative is "I'm poor anyway." The anterior cingulate cortex shows reduced error-detection capacity, allowing gross misalignment between financial reality and perception to persist without generating corrective action. Often, early messages about worthiness, family financial trauma, or experiences of sudden financial loss have created deep encodings that link financial safety to shame or unworthiness.
Our technique directly recalibrates the anterior insula's perception of financial status by repeatedly exposing it to actual financial data while neutralizing the shame-affect that usually accompanies money-awareness. We reprogram the medial prefrontal cortex's equation of net-worth with self-worth, untangling financial safety from identity-value. We restore the ventromedial prefrontal cortex's capacity to update threat-assessment when presented with objective financial evidence. We recalibrate the nucleus accumbens so genuine financial security becomes neurochemically rewarding, and image-maintenance spending loses its dopamine-appeal. We strengthen the anterior cingulate's error-detection so financial reality-checking becomes automatic. We address early trauma or messages that encoded money with shame and reprogram those pathways. You experience rapid restoration of accurate internal perception of your actual financial state, elimination of the shame-affect that distorts financial awareness, aligned decision-making where behavior matches reality rather than internal distortion, and genuine internal experience of financial security that matches objective reality.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Money Scripts - Unconscious Beliefs & Inherited Financial Programming
This could be your breakthrough. Let's do this!
Your financial behaviors are being driven by invisible scripts inherited from your family's relationship with money—scripts you never consciously chose. Money scripts are deeply ingrained, largely unconscious beliefs about money that were developed in childhood through observation, messaging, and experience. Common scripts include: (1) Money Avoidance—belief that money is evil or morally problematic, that you don't deserve wealth, or that discussing money is taboo; (2) Money Worship—belief that more money will solve all problems, that wealth equals happiness and acceptability, or that life value is determined by financial status; (3) Money Status—equation of net worth with self-worth, where financial success becomes proof of personal adequacy and financial struggle becomes proof of failure; and (4) Money Vigilance—excessive alertness to financial danger, inability to trust or enjoy wealth, constant scanning for financial threat, inability to delegate or spend even on needs. These scripts operate at unconscious neurological levels, driving financial decisions, risk-tolerance, saving patterns, spending patterns, and relationship dynamics around money.
The neurobiological mechanism involves neural encoding in the ventromedial prefrontal cortex and posterior cingulate cortex (regions that represent self and integrated identity) where financial beliefs have become fused with identity-core. The beliefs were encoded during childhood when the developing brain was maximally plastic and when parental modeling and messaging directly shaped limbic system organization. The nucleus accumbens became conditioned to associate specific financial behaviors with reward or punishment based on parental messages—money-avoidance may have been rewarded with parental approval, money-worship with dopamine-hits from consumption, money-status with validation, money-vigilance with safety-through-control. The anterior cingulate cortex encodes the script as a fundamental rule of how the world works, creating resistance to evidence that contradicts the script. The amygdala becomes hyperactive to financial situations that violate the script—money-avoiders become anxious when acquiring money, money-worshippers panic without continuous consumption, money-status people experience shame in non-wealthy contexts, money-vigilant people cannot relax around financial management. These scripts often remain invisible to the person—they feel like truth rather than programming—and efforts to change financial behavior fail because the script remain neurologically active.
Our technique makes the invisible scripts visible and then reprograms them at the neurological level. We identify the specific money scripts operating (often multiple simultaneous scripts in conflict), trace them to their childhood origins, and then systematically decondition the limbic system's responses to money-related situations. We reprogram the ventromedial and posterior cingulate so financial situations no longer trigger identity-threat responses. We recalibrate the nucleus accumbens so healthy financial behaviors generate genuine reward. We restore the anterior cingulate's capacity to hold nuanced understandings of money that transcend the limiting script. We help the amygdala develop accurate threat-assessment around financial situations. We establish new neural patterns where your financial decisions are driven by your actual values and goals rather than inherited unconscious programming. You experience clarity about previously invisible financial scripts, freedom from script-driven automatic reactions, capacity to make conscious financial decisions aligned with actual values, integration of multiple money-perspectives without internal conflict, and genuine enjoyment of financial security without the contamination of script-related shame or fear.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Screen Addiction and Digital Compulsivity
This could be your breakthrough. Let's do this!
Your dopamine pathways learned that the screen is the most rewarding place on earth. It's time to restore balance. Screen addiction (behavioral addiction to digital devices, social media, gaming, or internet) is characterized by compulsive use of screens despite negative consequences, loss of control over usage, tolerance (requiring increasing amounts of use), and withdrawal symptoms when access is restricted. Individuals with screen addiction experience damaged relationships, academic and work performance decline, sleep disruption, physical health impacts, and profound difficulty disengaging from devices. Screen addiction is particularly prevalent in adolescents whose developing brains are especially vulnerable to reinforcement mechanisms.
The neurobiological mechanism involves hijacking of the dopamine reward system by algorithmic platforms specifically engineered to maximize engagement and reward intensity. The apps and platforms exploit the brain's natural reward learning systems through variable ratio reinforcement schedules (random rewards increase engagement more than predictable ones), social proof mechanisms, and notifications designed to interrupt and recapture attention. The amygdala becomes hypersensitive to 'fear of missing out' (FOMO), and dopamine becomes dysregulated, leading to craving for screen engagement as a way to manage anxiety and emotional distress. The prefrontal cortex loses regulatory capacity as impulse control deteriorates.
Our technique recalibrates the reward system and restores executive capacity through targeted limbic intervention. We dissolve the algorithmic hijacking and restore genuine dopamine sensitivity where natural rewards become accessible again. Compulsive screen use transforms into balanced, conscious technology engagement. This isn't screen time limiting or willpower training. It's recoding of how your nervous system processes digital rewards and manages FOMO-based anxiety. You access freedom and restored capacity for non-digital engagement and relationships.
Related condition: For adolescent-specific screen addiction during critical developmental windows, see Teen Screen Addiction & Digital Escapism.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Trauma, Crisis & Personality Pathology
Rape & Sexual Assault
This could be your breakthrough. Let's do this!
Your body was violated and your nervous system learned that intimacy, vulnerability, or specific triggers equal survival danger. Sexual assault became encoded as core threat. Rape and sexual assault survivors experience profound psychological consequences including PTSD, complex trauma, hypervigilance, dissociation, shame, difficulty with trust and intimacy, intrusive memories, and often suicidal ideation. The assault violated bodily autonomy and safety, and the nervous system remains in protective shutdown anticipating recurrence. Many survivors struggle with sexuality, intimacy, and recovery despite desperately wanting to reclaim their lives and bodies.
The neurobiological mechanism involves amygdala sensitization to assault-related trauma cues (locations, smells, physical sensations, interpersonal closeness) where exposure to trauma reminders triggers full threat-response as if assault is currently occurring. The hippocampus becomes dysregulated, fragmenting trauma memories so they remain intrusive and unprocessed. The anterior cingulate cortex generates persistent error-checking and threat-scanning. Dissociation occurs as a protective response where consciousness disconnects from body sensation during intimacy or vulnerability. The insula loses accurate interoceptive awareness, making the body feel unsafe or unowned. The medial prefrontal cortex encodes the assault as self-defining, creating shame and identity damage. Sexual arousal becomes associated with danger rather than pleasure.
Our technique systematically processes the trauma encoding and restores felt safety in the body through targeted trauma-specific limbic intervention. We desensitize trauma triggers and restore accurate threat-assessment. Your nervous system regains capacity to distinguish assault threat from current safety. You experience reclaimed body ownership, restored capacity for intimacy and pleasure, freedom from intrusive trauma memories, and integration of the assault as something that happened to you rather than something that defines who you are.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.PTSD - Post-Traumatic Stress Disorder
This could be your breakthrough. Let's do this!
Your amygdala is running an outdated threat-detection protocol. It's time to install the current version. Post-Traumatic Stress Disorder develops following exposure to a traumatic event involving actual or threatened death, serious injury, or violence, resulting in intrusive memories, avoidance behaviors, and persistent alterations in mood and cognition. PTSD sufferers often experience flashbacks that feel as vivid and real as the original trauma, causing them to re-experience the event with full physiological activation of the fight-or-flight response.
The neurobiological mechanism of PTSD involves a failure of the brain's threat-extinction system where new, contradictory information fails to update stored trauma memories. Anxiety locks the limbic system into a chronic state of hyper-arousal where the amygdala becomes hyper-responsive to triggers, causing the prefrontal cortex to lose its ability to regulate 'false alarms.' This increases the frequency of flashbacks and dissociative episodes where individuals feel disconnected from their body or surroundings. The brain essentially becomes stuck in a state of perpetual danger even when objective safety is present.
Our technique recodes the threat-detection and memory-processing systems through creative limbic recalibration. We identify the triggering belief patterns and amygdala hijacks that maintain the traumatic loop, then replace them with updated threat-assessment protocols. This is not talk therapy, EMDR, or reliving the trauma. It is precision recoding of how your brain processes the memory and threat signal. Flashbacks recede, triggers lose their charge, and you access genuine presence and safety.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Developmental Trauma (Childhood Trauma)
This could be your breakthrough. Let's do this!
The brain that survived cannot become the brain that thrives without a radical recalibration of survival coding. Developmental trauma (also known as Complex PTSD or Childhood Trauma) occurs when a child experiences repeated or prolonged adversity such as neglect, abuse, or violence during critical periods of brain development. Unlike single-incident trauma, developmental trauma shapes the fundamental architecture of the brain before the prefrontal cortex fully matures. Children exposed to these adverse experiences often develop hypervigilance, difficulty trusting others, emotional dysregulation, and challenges with identity formation that persist into adulthood.
The neurobiological impact is profound: adverse early experiences lock the developing brain into a state of limbic dominance where survival circuits override development of higher-order thinking. Chronic anxiety prevents the maturation of the prefrontal cortex and creates a permanent 'hyper-arousal' loop where the amygdala overreacts to neutral environmental cues as if they were life-threatening. The brain essentially becomes wired for threat-detection rather than growth and learning, making it difficult for individuals to feel safe even in secure environments.
Our technique targets these ancient survival blueprints through creative reprogramming of the limbic system. We identify the limiting beliefs and dangerous assumptions your brain learned to keep you alive, then replace them with new neural patterns of safety and possibility. This is not reliving trauma or gradual desensitization. It is precision recoding of the threat-detection and trust systems. You access genuine safety and belonging through rewired nervous systems.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Cult Recovery and Religious Trauma - Fear of Damnation
This could be your breakthrough. Let's do this!
Your nervous system was programmed to fear cosmic punishment. Recovery requires recoding the existential threat system. Cult recovery and religious trauma encompass psychological injury sustained through involvement in high-control groups or religious systems that use shame, fear of damnation, thought control, and spiritual manipulation to maintain obedience. Individuals recovering from cult involvement or fundamentalist religious trauma experience profound anxiety about divine punishment or damnation, shame about their sexuality or autonomy, identity confusion following loss of prescribed identity, and difficulty trusting their own judgment. Complex PTSD is common, with religious concepts (sin, hellfire, divine judgment) triggering severe anxiety and dissociation.
The neurobiological mechanism involves systematic amygdala conditioning where existential fear responses became paired with specific religious concepts, creating a state where thinking certain thoughts or experiencing certain desires (sexuality, questioning, independence) triggers existential threat experience of cosmic punishment. The insula becomes hyperactive to shame and sin-related thoughts. The prefrontal cortex loses capacity to evaluate religious teachings rationally, as the limbic system overrides logical processing with fear-based imperatives. The moral decision-making networks become hijacked by learned fear associations. The nervous system remains trapped in a state where autonomy and authentic self-expression trigger fear of divine punishment.
Our technique systematically deconditions the amygdala's association between autonomy, sexuality, questioning, and cosmic threat through targeted limbic intervention. We restore prefrontal regulation of fear-based religious programming and dismantle shame-based conditioning. Religious autonomy, authentic self-expression, and sexuality no longer trigger threat response. This isn't deprogramming or religious argument. It's recoding of how your nervous system processes spiritual concepts and threat. You access genuine spiritual freedom, restored autonomy, and authentic identity integration.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Financial Flashpoint Trauma - Catastrophic Financial Events & Lasting Financial PTSD
This could be your breakthrough. Let's do this!
Your nervous system was traumatized by a financial catastrophe—bankruptcy, business collapse, sudden job loss, foreclosure, homelessness—and now your amygdala is locked in hypervigilance about financial security that no amount of current stability can quiet. A financial flashpoint is a traumatic financial event such as bankruptcy, sudden job loss, loss of a home, business failure, or sudden displacement that creates a lasting psychological scar and establishes trauma-level encoding of financial threat. Unlike ordinary financial stress, financial flashpoint trauma involves acute loss of identity (for business owners), home, security, and future certainty all at once. The trauma creates lasting psychological effects: compulsive hoarding or avoidance of financial planning, inability to make financial decisions despite understanding the need, hypervigilance about every financial marker, intrusive thoughts about financial catastrophe, startle-response to financial reminders, avoidance of banking or financial engagement, or conversely, obsessive money-management that never feels sufficient. The person's nervous system remains encoded in "financial security is fragile and can be destroyed instantly," preventing the normal relaxation into financial stability even when it has been re-established.
The neurobiological mechanism involves traumatic encoding of financial events in the amygdala and insula, combined with dysregulation of the threat-assessment systems. The amygdala has encoded financial events (particularly specific triggers like losing a job, receiving a foreclosure notice, or watching savings disappear) as acute threat equivalent to mortal danger. The anterior insula generates persistent bodily threat-signals in response to financial reminders—racing heartbeat, nausea, or panic in response to seeing numbers on bank statements or receiving financial communications. The ventromedial prefrontal cortex's threat-appraisal system has been recalibrated and remains locked in the belief "financial security is impossible" despite objective current stability. The dorsolateral prefrontal cortex shows reduced capacity for rational financial planning because cognitive resources are redirected toward threat-scanning. The default mode network generates repetitive fearful narratives about future financial catastrophe. The hippocampus may show dysregulation in the integration of new financial stability-information—the person's episodic memory remains locked in the catastrophe event rather than updating to current reality.
Our technique involves dual-layer recalibration: (1) traumatic encoding resolution in which the specific financial traumatic memories are processed and the amygdala's threat-encoding is neutralized through direct limbic recalibration without exposure; and (2) threat-appraisal system recalibration in which the ventromedial prefrontal cortex's belief in inevitable financial catastrophe is reprogrammed through direct nervous system work and integration of new stability-information. We recalibrate the anterior insula's bodily threat-signals so financial reminders and communications no longer generate survival-mode activation. We restore the dorsolateral prefrontal cortex's capacity for rational financial planning and executive function. We reprogram the default mode network's narrative from "catastrophe is inevitable" to "I have survived and can maintain stability." We help the hippocampus integrate new positive financial experiences to update the memory-system away from exclusive focus on the traumatic event. We address any behavior patterns (hoarding, avoidance, compulsive checking) that developed as protective responses and reprogram them. You experience rapid elimination of trauma-related hypervigilance and panic in financial situations, restored capacity for rational financial planning and decision-making, elimination of compulsive or avoidant financial behaviors, ability to build and maintain financial security without the intrusive terror of impending catastrophe, integration of past trauma while building authentic future security, and genuine internal experience of financial stability that matches objective reality.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Moral Injury - Values Violation
This could be your breakthrough. Let's do this!
You acted or witnessed actions that betrayed your core values. Your nervous system now encodes that betrayal as self-threat and shame. Moral injury is a profound psychological response to perpetrating, witnessing, or failing to prevent violations of one's deeply held moral beliefs and values. Unlike trauma (which involves threat to survival), moral injury involves threat to one's identity and sense of self as a good person. Individuals with moral injury experience persistent guilt, shame, rage at self or others, loss of meaning, and difficulty trusting themselves or the world.
The neurobiological mechanism involves the medial prefrontal cortex—which maintains identity and values—encoding the value-violating action or inaction as a core identity threat. The amygdala becomes conditioned to respond to reminders of the moral violation with intense shame and not-self states. The ventromedial prefrontal cortex fails to integrate the violation into a coherent identity, leaving it in a fragmented, shame-laden state. Rumination about the moral violation becomes encoded as a core feature of identity, and the nervous system perpetually re-experiences the shame of the value violation. The wound is to one's sense of self as moral.
Our technique integrates the moral violation into a coherent, compassionate identity narrative through targeted limbic and identity work. We dissolve the shame-encoding and restore wholeness of self. Your nervous system ceases to treat the moral violation as defining your identity. You experience integrated self-understanding, restored capacity for self-compassion, and renewed sense of meaning and values.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Hyper Cynicism - Depressive Realism, Pervasive Distrust & Defensive Negativity
This could be your breakthrough. Let's do this!
Your nervous system may have decided that hope is what gets people hurt. Hyper cynicism is not ordinary skepticism or healthy discernment. It is a rigid, overlearned interpretive stance in which the mind narrates people, systems, motives, and future outcomes through a lens of betrayal, futility, corruption, or inevitable disappointment. The person may feel that they are simply being "realistic" while everyone else is naive, sentimental, or self-deceived. In some individuals this resembles what has been called depressive realism: a stark, linear, bias-stripped view of life in which optimism feels dishonest and cynicism feels like truth. In more severe or personality-structured forms it can overlap with pervasive distrust, including paranoid predictions of betrayal or harm, or schizoid-style detachment where cynicism functions as a defensive wall against the vulnerability of social connection. This stance is often a compensation for the opposite pole: when defensive idealization, wish-based thinking, or naive trust has previously exposed the person to humiliation, exploitation, betrayal, or moral injury, the mind may swing into hyper cynicism to make sure openness never becomes that dangerous again. In workplace variants, the same stance gets projected onto employers, leadership, missions, customers, or the entire concept of meaningful work, especially after chronic overextension, hypocrisy exposure, or repeated exploitation. In relationship variants, the nervous system may begin treating intimacy itself as a setup for disappointment, using sarcasm, suspicion, emotional distance, or preemptive contempt to avoid dependence, grief, or humiliation. It is also common in occupational burnout, where chronic overtaxing leads to emotional distance, negativism, and contempt for the entire work system, and in moral injury, where the person begins to interpret future people and institutions through a hardened lens designed to prevent ever being fooled or violated again.
The neurobiological mechanism involves chronic threat-based prediction dominating interpretation. The amygdala and salience systems bias attention toward evidence of danger, hypocrisy, incompetence, betrayal, or collapse. The anterior cingulate cortex remains over-engaged in error-detection and contradiction-monitoring, constantly scanning for what is wrong or unsafe. The ventromedial prefrontal cortex develops hardened beliefs such as "people always disappoint," "systems are rigged," "every relationship ends in betrayal," or "hope is for fools," and then uses those beliefs to interpret new information before it is fully evaluated. The dorsolateral prefrontal cortex may construct elaborate justifications for the cynical stance, making it feel intellectually superior rather than emotionally defended. The insula tags interpersonal contact, institutions, work obligations, and future-oriented thinking with disgust, dread, or deadness rather than curiosity or possibility. In many cases this is a compensatory correction against a prior history of overtrust, idealization, or denial: the nervous system learns that if it expects the worst, it cannot be fooled in the same way again. In burnout, the PFC narrates chronic limbic exhaustion as the uselessness of the work, the mission, or the people involved. In relationship-focused variants, attachment cues themselves become fused with anticipated disappointment, engulfment, betrayal, or ridicule, so distance starts feeling safer than tenderness. In moral injury, future trust is filtered through the memory of value-violation so the organism is never caught undefended again. What looks like philosophical realism is often a nervous system that no longer feels safe enough to generate openness, trust, or adaptive optimism.
Our technique targets the threat-prediction machinery beneath the cynical narrative. We recalibrate the amygdala's reflexive expectation of betrayal, restore flexibility to the ventromedial prefrontal cortex's world-models, and reduce the anterior cingulate's compulsive fixation on what's wrong, corrupt, or doomed. We help the insula distinguish true danger from habituated negativism and re-open access to social, relational, vocational, and existential engagement without forcing fake positivity. This is not an attempt to make someone gullible, compliant, or blind to genuine corruption. It is the restoration of discernment without totalized distrust. You experience less compulsive negativism, reduced need to protect yourself through contempt or emotional distance, greater capacity to evaluate people, work systems, and intimate relationships realistically without collapsing into bitterness, and a nervous system that no longer mistakes openness for danger or cynicism for truth itself.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Defensive Idealization - Unrealistic Optimism, Reality Avoidance & Wish-Based Thinking
This could be your breakthrough. Let's do this!
Your nervous system may have decided that the only tolerable future is the one it beautifies, sanitizes, or spiritually guarantees. Defensive idealization is the opposite pole of hyper cynicism. Instead of anticipating betrayal, collapse, or disappointment, the mind overcorrects toward unrealistic optimism, selective attention to reassuring signs, and a refusal to metabolize contradictory evidence. This is not grounded hope, resilience, or mature faith. It is an overlearned protective style in which danger gets minimized, motives get idealized, and complexity gets replaced with certainty that "everything will work out" if one just stays positive, trusts hard enough, or refuses to look directly at what is happening. In some individuals it appears as chronic denial, in others as relational idealization, redemptive certainty, suggestibility to charismatic personalities, or wish-based thinking that treats desire as evidence. This stance is often a compensation for the opposite pole: when hyper cynicism, chronic distrust, or repeated anticipation of betrayal has become unbearable, the mind may swing toward idealization, magical reassurance, and naive faith because certainty feels safer than living in permanent suspicion. This can create unusual vulnerability to narcissists, conmen, manipulative gurus, apocalyptic belief systems, superstition, and rigid religiosity, because the person's need for reassurance outruns their reality-testing. In more spiritualized forms it can resemble spiritual bypassing, where grief, anger, accountability, and skepticism are skipped in favor of destiny narratives, miraculous explanations, prophetic certainty, or the conviction that discernment itself is a lower form of consciousness.
The neurobiological mechanism involves top-down inhibition of threat information rather than healthy integration of it. The ventromedial prefrontal cortex generates overly coherent positive narratives that suppress disconfirming evidence before it can fully update the model of reality. The anterior cingulate cortex becomes less willing to sustain contradiction, ambiguity, or error-signals, so the person exits uncertainty too quickly and lands in premature reassurance. The dorsolateral prefrontal cortex may become recruited into rationalization, constructing polished explanations for why obvious risks do not apply, why boundaries are unnecessary, why a charismatic person must be trustworthy, or why improbable claims should be accepted because they feel meaningful. The amygdala's warnings may be chronically bypassed, numbed, or reinterpreted as mere negativity rather than useful data. The insula's uncomfortable signals of dread, aversion, or intuition are overruled by a learned mandate to stay uplifted, surrendered, faithful, or certain. In many cases this is a compensatory correction against a prior state of bitterness, suspicion, or collapse into distrust: the nervous system reaches for idealization because unbuffered cynicism feels intolerable. In relationship variants, it can appear as idealizing unavailable, exploitative, or grandiose partners, dismissing red flags as tests of love or faith, and repeatedly converting manipulation into a redemption story. In spiritual or superstitious variants, coincidence gets over-read as destiny, authority gets confused with wisdom, and the need for cosmic safety can override evidence, boundaries, and independent judgment. What looks like positivity is often a nervous system that cannot yet tolerate grief, disillusionment, uncertainty, or the pain of seeing clearly.
Our technique restores contact with reality without collapsing the person into despair or cynicism. We help the nervous system tolerate ambiguity, loss, and contradiction so optimism no longer has to be inflated into denial. We recalibrate the ventromedial prefrontal cortex's need for redemptive certainty, strengthen the anterior cingulate's capacity to stay with disconfirming evidence, and restore the insula's role as a source of valid internal warning rather than something to override with affirmations, prophecy, or charm. This is not an attack on hope, meaning, spirituality, or genuine faith. It is the restoration of grounded hope that can face facts. You experience less compulsive idealization, reduced susceptibility to manipulators and grandiose personalities, greater ability to distinguish trust from fantasy and reverence from submission, clearer perception of red flags without collapsing into paranoia, and a nervous system that no longer mistakes denial for faith or wish-based thinking for wisdom.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Trauma, Drama & Related
This could be your breakthrough. Let's do this!
Life experiences imprinted your nervous system with threat patterns that now generate chronic survival responses. Whether psychological trauma, relational trauma, complex trauma, or recurrent destructive patterns, your nervous system learned the world is dangerous. Trauma, drama, and related patterns encompass psychological outcomes from negative life experiences including PTSD, complex PTSD, trauma-related anxiety, recurrent harmful relationship patterns, crisis-prone lifestyle, and chronic survival-state activation. Individuals often unconsciously recreate traumatic patterns or remain stuck in threat-detection despite current safety.
The neurobiological mechanism involves amygdala sensitization and conditioning to trauma-related cues, where the nervous system continues responding as if threat persists long after actual danger has passed. The hippocampus becomes dysregulated, preventing proper time-stamping and integration of trauma memories, leaving them fragmented and intrusive. The prefrontal cortex loses regulatory capacity over the amygdala during trauma-reminder exposure. The ventromedial prefrontal cortex fails to maintain accurate threat assessment, leading to generalization where anything resembling trauma context becomes a threat trigger. The nervous system becomes locked in a protective hypervigilance that was once adaptive but now becomes constraining.
Our technique systematically desensitizes trauma encoding and restores accurate threat-assessment through targeted limbic intervention. We process trauma memories and diminish their emotional charge and salience. Your nervous system regains capacity to distinguish past threat from present safety. You experience freedom from intrusive trauma memories and chronic threat-detection, restored capacity for trust and genuine engagement with life.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Narcissistic Personality Disorder - Pathological Pride & Grandiosity
This could be your breakthrough. Let's do this!
Your nervous system learned that you are special, exceptional, and above the normal rules that bind ordinary people. Narcissism is your survival strategy. Narcissistic Personality Disorder (NPD) is characterized by a pervasive pattern of grandiosity (in fantasy or behavior), a deep need for excessive admiration and attention, and a profound lack of empathy for others' experiences and needs. Individuals with NPD experience inflated self-importance, require constant attention and validation, become rageful in response to criticism, exploit others without guilt, and maintain shallow relationships in which others are valued only for their utility to the narcissist. The narcissistic person often achieves external success but experiences profound internal emptiness when not receiving admiration.
The neurobiological mechanism involves a fundamental dysregulation of the brain systems responsible for self-other integration and empathy. The medial prefrontal cortex (self-referential processing) is hyperactive and locked into self-focus—the narcissist's neural activity patterns show reduced connectivity between brain regions necessary for understanding others' mental states (Theory of Mind circuits). The insula (empathic resonance with others' distress) shows reduced activation—the narcissist's brain literally doesn't activate when seeing others suffer, making empathic concern neurologically unavailable. The ventromedial prefrontal cortex fails to generate accurate self-worth feedback from internal sources, creating a desperate dependence on external admiration to regulate self-esteem. When admiration is threatened, the amygdala becomes hyperactive in threat-response (narcissistic rage is a genuine neurological emergency response, not calculated manipulation). The orbitofrontal cortex (decision-making about others' needs vs. self-interest) becomes dysregulated around prioritizing self-interest at others' expense without guilt activation.
Our technique recalibrates the medial prefrontal cortex's hyperactive self-focus and rebuilds the neural circuits for other-referential thinking and genuine empathy. We activate the insula's capacity to resonate with others' suffering, replacing the neurological absence of empathic concern. The ventromedial prefrontal cortex learns to generate intrinsic self-worth independent of external admiration, reducing the desperate reliance on narcissistic supply. The amygdala recalibrates to recognize that criticism and limitation are not existential threat. The orbitofrontal cortex rebuilds genuine capacity to weigh others' needs alongside self-interest. You experience profound internal worth independent of admiration, genuine capacity for authentic relationships based on reciprocal regard, freedom from narcissistic rage when facing limitation, and genuine empathy activation where others' suffering becomes meaningful.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Antisocial Personality Disorder - Pathological Deception & Manipulation
This could be your breakthrough. Let's do this!
Your nervous system learned early that predatory dominance is the path to survival and that other people are tools to be used without regard for their wellbeing. Antisocial Personality Disorder (ASPD) is characterized by a pervasive pattern of violation of others' rights that begins in childhood and includes deceitfulness (pathological lying, conning others for personal gain), impulsivity or poor planning, irritability or aggression, reckless disregard for safety of self or others, consistent irresponsibility, and crucially, lack of remorse after harming others. Individuals with ASPD manipulate, exploit, and sometimes violently assault others while experiencing little to no guilt or empathic concern about the harm they cause. The person may be charming and superficially engaging (using these skills to manipulate), but beneath the surface is a fundamentally self-centered nervous system incapable of authentic reciprocity.
The neurobiological mechanism involves profound dysregulation of the empathy and conscience systems combined with enhanced reward sensitivity to dominance and exploitation. The insula and anterior cingulate cortex (crucial for empathic resonance with others' suffering and guilt generation) show reduced activation—the person's brain literally doesn't activate when viewing others' distress, making empathic concern neurologically unavailable. The ventromedial prefrontal cortex fails to generate guilt or shame in response to harm-causing, and fails to encode others' wellbeing as having personal value. The orbitofrontal cortex (decision-making) becomes hyperactive in pursuing dominance and exploitation, with reduced connectivity to regions responsible for considering others' perspectives. The amygdala shows reduced fear-response to punishment, making consequences less deterrent. The nucleus accumbens becomes hyperresponsive to rewards from dominance, deception success, and exploitation, making predatory behavior neurochemically rewarding. Early trauma, neglect, or abuse often contributes to the neural development that creates this pattern—the person learned that others cannot be trusted and exploitation is the only safe strategy.
Our technique begins by activating the dormant neural circuits for empathic resonance and guilt-generation through intensive limbic intervention and experiential exposure to the genuine consequences of harm-causing. We rebuild the ventromedial prefrontal cortex's valuation of others' wellbeing through confrontation with the reality of harm caused and the human cost of exploitation. We recalibrate the orbitofrontal cortex's reward-sensitivity away from dominance-seeking toward reciprocal relationship. We activate genuine consequence-awareness in the amygdala's threat-detection. This work requires genuine motivation to change—without internal motivation, the person's sophisticated manipulation skills and lack of remorse make therapeutic change unlikely. When change occurs, you experience awakening of genuine empathic concern for others' suffering, reduced impulsive exploitation as alternative reward-pathways activate, capacity for authentic reciprocal relationships beyond manipulation, and integration of conscience where others' suffering becomes genuinely important.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Pathological & Compulsive Lying - Factitious Identity, Pseudologia Fantastica & Habitual Deception
This could be your breakthrough. Let's do this!
Your nervous system has organized itself around deception as the primary survival mechanism, whether through automatic, compulsive lie-generation or through constructing and living within an elaborate false identity. Pathological and compulsive lying encompass a spectrum of deceptive patterns: (1) Compulsive lying (pseudologia fantastica), where your brain automatically generates frequent, elaborate lies without clear external motivation, often about mundane details as well as significant events, occurring even when the truth would be simpler or safer; and (2) Pathological lying, where you have constructed and persistently maintained an extended false identity or life story across multiple contexts and relationships—complete with false credentials, fabricated accomplishments, invented relationships, or fictional trauma—sometimes believing your own false narratives completely. Both patterns involve loss of control, distress about the pattern, serious life consequences, and profound underlying threats to honest self-disclosure. Some individuals experience primarily automatic impulsive lying; others develop organized false identities; many experience both simultaneously with different lies serving different defensive functions.
The neurobiological mechanisms are closely related across both presentations. The ventromedial prefrontal cortex fails to maintain adequate distinction between actual experiences and constructed narratives, and becomes hyperactive in self-protection (generating lies as automatic anxiety-reduction). The anterior cingulate cortex (error-detection and impulse-inhibition) shows dysregulation—either hyperactive-but-ineffective at stopping lies or hypoactive and allowing false narratives to maintain persistent activation without constant reality-checking. The nucleus accumbens becomes dopamine-responsive to the lie-generation or false-identity-maintenance process itself—the creative process of constructing false narratives becomes neurochemically rewarding, independent of external gain. The medial prefrontal cortex (self-representation and autobiographical memory) becomes dysregulated, with constructed narratives sometimes more psychologically vivid than accurate experiences. The insula shows either hyperactivity in resistance to vulnerable truth-telling (truth becomes encoded as dangerous exposure) or reduced interoceptive awareness disconnecting the person from authentic internal states. The posterior cingulate cortex and precuneus (autobiographical identity regions) show dysregulation, allowing false narratives or identities to compete with actual memory and self-representation. The amygdala has encoded threat-associations with honesty (early experiences where truth-telling resulted in punishment, shame, rejection, or abandonment) and may show hyperactive threat-response to exposure of lies or revelation of the actual self. In pathological lying presentations, the medial prefrontal cortex becomes bifurcated with reduced neural integration between the false identity and actual experience, creating dissociation. Across both patterns, profound underlying shame, identity fragmentation, early relational trauma, and learned patterns that made authentic self-disclosure feel threateningly dangerous drive the compulsive or organized deception. The difference lies partly in temporal scope (impulsive moment-to-moment lies vs. sustained identity-level deception) and neuropsychological mechanisms (working-memory vs. identity-encoding systems), but the root threat-association with honesty is consistent.
Our technique recalibrates the entire truth-deception reward-and-threat system. We reprogram the ventromedial prefrontal cortex so truth-telling is encoded as genuine safety rather than danger, and so the person can tolerate vulnerability without defaulting to narrative falsification. We strengthen the anterior cingulate's reality-monitoring and impulse-inhibition, creating functional 'brakes' on automatic lie-generation and clarity about what is actual vs. constructed. We recalibrate the nucleus accumbens so authentic truth-telling, genuine achievement, and authentic relational connection become neurochemically rewarding—greater dopamine-response to truth and genuine connection than to lie-generation or false-identity maintenance. We help the insula tolerate authentic self-disclosure and reconnect with genuine internal states. We recalibrate the posterior cingulate and precuneus so autobiographical memory stabilizes around actual experiences. We address the amygdala's threat-associations with honesty, neutralizing early traumas that made truth-telling dangerous. If bifurcated identity is present, we progressively integrate actual and false self-representations so you can tolerate inhabiting your actual identity. We address the profound shame and unworthiness beliefs that made deception feel necessary. You experience dramatic reduction in lie-generation (both impulsive and organized), dissolution of false identity investments, increased capacity for authentic self-disclosure and genuine vulnerability, relief from the cognitive labor of maintaining deception, genuine relational connection based on authenticity, and development of solid self-worth rooted in actual accomplishment and genuine interiority.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Histrionic Personality Disorder - Attention-Seeking & Dramatic Performance
This could be your breakthrough. Let's do this!
Your nervous system learned that your survival depends on being the center of attention and that dramatic emotional expression and strategic vulnerability are the tools that guarantee others will remain focused on you. Histrionic Personality Disorder (HPD) is characterized by a pervasive pattern of excessive emotionality and attention-seeking, including discomfort when not the center of attention, provocative or sexualized behavior, rapidly shifting and shallow emotions, theatrical or exaggerated emotional expression, use of physical appearance to draw attention, and a manner of speech that is impressionistic and lacks detail. Individuals with HPD fabricate or dramatically exaggerate illnesses, injuries, or personal traumas to maintain attention and sympathy. Unlike antisocial individuals who lie for manipulation and gain, histrionic individuals lie to maintain their central position in the relational drama—the lie itself is less important than the attention and emotional response it generates.
The neurobiological mechanism involves dysregulation of the reward system specifically around social attention and validation, combined with emotional dysregulation and identity instability similar to BPD but driven by different primary needs. The nucleus accumbens becomes hyperresponsive to attention and approval, making the person neurochemically dependent on being the center of social focus. The medial prefrontal cortex (self-concept) becomes unstable and primarily defined by reflected appraisals—the person's sense of self is contingent on how others perceive them, and they will dramatically shift their presentation to maintain positive attention. The insula becomes dysregulated in emotional intensity—emotions are experienced as overwhelming and dramatic, and the person uses theatrical emotional expression both to process their internal states and to guarantee others' emotional investment in them. The ventromedial prefrontal cortex fails to maintain genuine continuity of identity across contexts—the person becomes whoever garners maximum attention in each situation. The anterior cingulate cortex becomes sensitized to any threat of being ignored or deprioritized, generating intense distress that drives increased dramatic behavior. Unlike narcissistic individuals (who need admiration of their superiority), histrionic individuals need emotional involvement, whether positive or negative—disapproval is preferable to being ignored.
Our technique recalibrates the nucleus accumbens's hyperactive attention-reward dependence and helps the person find dopamine-satisfaction in authentic connection rather than attention-capture. We stabilize the medial prefrontal cortex's unstable self-concept and build identity rooted in genuine values and preferences rather than relational performance. We help the insula learn to tolerate emotional experience without requiring dramatic expression for processing. We recalibrate the anterior cingulate's hypersensitivity to being ignored. We address the underlying terror of invisibility or irrelevance that drives the attention-seeking. You experience more stable sense of self across contexts, reduced dependency on external attention and approval, capacity for authentic relationships not driven by attention-maintenance, emotional expression that communicates genuine feeling rather than performing for effect, and the relief of being seen and valued for your actual self rather than your dramatic presentation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Avoidant Personality Disorder - Cowardice & Social Withdrawal
This could be your breakthrough. Let's do this!
Your nervous system learned that social exposure is unbearable danger and that withdrawing is the only way to survive the crushing fear of rejection. Avoidant Personality Disorder (AVPD) is characterized by a pervasive pattern of social inhibition, feelings of inadequacy, and extreme hypersensitivity to negative evaluation or rejection. Individuals with AVPD avoid social interaction, career advancement, intimate relationships, and activities outside their comfort zone not because they lack "courage" but because the amygdala generates such intense rejection-terror that avoidance feels necessary for survival. The person wants connection but the fear of rejection far outweighs the motivation to engage. This creates a trapped existence where the person becomes increasingly isolated, missing opportunities and relationships, while internally feeling branded as fundamentally unworthy and inadequate.
The neurobiological mechanism involves pervasive amygdala hyperactivity in social threat-detection combined with ventromedial prefrontal cortex failure to generate accurate self-worth. The amygdala has become sensitized to perceive any possibility of social evaluation as threat requiring escape. The anterior insula becomes hyperresponsive to signs of rejection or disapproval, generating unbearable social pain. The medial prefrontal cortex encodes the self as fundamentally unworthy ("If they really know me, they will reject me"). The dorsolateral prefrontal cortex loses capacity for social risk-taking when rejection-fear activates. Unlike social anxiety (where the person is anxious but tries to engage), AVPD involves internalized conviction of unworthiness that makes approach behavior feel pointless or dangerous. The nucleus accumbens becomes dopamine-depleted around social engagement, losing the reward that would normally motivate social connection. The person becomes locked in an avoidance pattern: avoidance temporarily reduces anxiety, but sustained avoidance reinforces the belief that social situations are genuinely dangerous.
Our technique recalibrates the amygdala's hyperactive rejection-detection and the insula's social pain intensity through targeted limbic intervention. We rebuild the medial prefrontal cortex's capacity to maintain self-worth independent of social approval. We systematically reduce the rewarded association between avoidance and anxiety-relief by gradually exposing the person to social situations while their limbic system recalibrates. The dorsolateral prefrontal cortex regains capacity for calculated social risk-taking. The nucleus accumbens relearns to find dopamine-reward in social connection. You experience decreased social anxiety where social situations become manageable, restored capacity to engage socially despite imperfection, genuine relationships based on authentic connection rather than avoidance of rejection, and the expansion of your world beyond the shrinking circle of isolation.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Borderline Personality Disorder - Chronic Envy & Unstable Self
This could be your breakthrough. Let's do this!
Your nervous system became convinced that you are fundamentally unworthy while simultaneously tortured by the conviction that others possess what you desperately lack. Borderline Personality Disorder (BPD) is characterized by a pervasive pattern of unstable and intense interpersonal relationships, unstable self-image, impulsive and self-harming behaviors, intense fear of abandonment, affective instability, and chronic feelings of emptiness. Individuals with BPD experience agonizing social comparison (intense envy of others' apparent wholeness and capability), desperate attempts to avoid abandonment leading to relationship deterioration, identity fragmentation where the self shifts dramatically based on relational context, and compulsive self-harm as a way to manage intolerable emotional pain that the person feels they deserve.
The neurobiological mechanism involves profound dysregulation of the emotional processing systems combined with a fragmented sense of self. The amygdala is hyperresponsive to perceived rejection or abandonment threats, generating intense abandonment terror and relationship-seeking desperation that often pushes people away. The ventromedial prefrontal cortex fails to maintain a coherent sense of self-worth across time—the person feels worthless one moment and adequate the next, creating internal instability that no external reassurance can resolve. The anterior insula becomes hyperactive in distress-signal generation—emotional pain reaches unbearable intensity, making self-harm feel necessary for pain regulation. The medial prefrontal cortex encodes unstable representations of both self and others—relationships are experienced as all-good or all-bad with no middle ground, and the self is experienced as fundamentally defective. Social comparison circuits become hyperactive, generating agonizing envy of others perceived as whole, capable, and worthy of love. The dorsolateral prefrontal cortex loses capacity for impulse inhibition when emotional pain reaches threshold, leading to cutting, substance abuse, reckless behavior, or crisis-seeking.
Our technique helps the amygdala recalibrate abandonment-threat perception and recognize that rejection is survivable and doesn't mean fundamental unworthiness. We rebuild the ventromedial prefrontal cortex's capacity to maintain a coherent, continuous sense of self across time and relational contexts. The insula recalibrates emotional pain perception—intense emotions become manageable rather than unbearable. The medial prefrontal cortex develops integrated self-concept that transcends relational context and incorporates both strengths and limitations without collapsing into worthlessness when limitations are exposed. The social comparison circuits recalibrate to recognize that others' success doesn't diminish personal worth. We develop genuine emotion-regulation alternatives to self-harm. You experience stable sense of self across contexts, capacity for relationships not driven by desperate abandonment-prevention, reduced chronic emptiness, ability to tolerate emotional pain without self-harm, and freedom from tormenting social comparison.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Identity, Culture & Prejudice
Sexual Orientation, Asexuality & Gender Identity Anxiety - Shame, Concealment & Self-Doubt
This could be your breakthrough. Let's do this!
Your nervous system may have learned that authentic identity is dangerous to reveal, question, or even feel. Sexual orientation and gender identity anxiety refers to chronic fear, shame, hypervigilance, concealment, or compulsive self-doubt surrounding one's sexual orientation, romantic orientation, asexuality-spectrum identity, or gender identity. This is not the identity itself being a disorder. The distress arises when a person has been taught that their internal reality is unsafe, unacceptable, invalid, or socially catastrophic. Individuals may obsessively question whether they are "really" who they think they are, fear rejection if known, experience panic about being judged by family or religion, or feel trapped between authenticity and belonging.
The neurobiological mechanism involves amygdala threat-conditioning around identity disclosure, desire, non-desire, embodiment, and social belonging. The insula becomes hypervigilant to bodily and relational cues, making every attraction, lack of attraction, gendered feeling, or interpersonal reaction feel diagnostic and high-stakes. This can affect people across the spectrum, including asexual individuals whose lack of sexual attraction is repeatedly pathologized, doubted, or pressured into explanation. The anterior cingulate fuels rumination and compulsive identity-checking, while the ventromedial prefrontal cortex may encode shame narratives such as "If this is true about me, I will lose love, safety, or legitimacy." The result is a loop of concealment, self-monitoring, reassurance-seeking, and minority-stress activation.
Our technique targets the threat-encoding around authentic identity rather than treating orientation, asexuality, or gender diversity as pathology. We help the nervous system uncouple authenticity from danger, reduce panic-based self-monitoring, and restore internal permission to exist without compulsive justification. This is not conversion work, ideological persuasion, or identity assignment. It is recalibration of the fear circuitry that turns self-knowledge into threat. You experience reduced shame, less compulsive self-doubt, greater capacity for clarity without panic, and a nervous system that no longer treats authentic identity as something to hide from or defend against at all times.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Homophobia, Transphobia, Sexual Orientation & Gender Identity Prejudice
This could be your breakthrough. Let's do this!
Your nervous system learned to perceive sexual orientation and gender diversity as threat requiring elimination or conversion. The amygdala hijack around sexuality and gender has become neurologically entrenched. Homophobia, transphobia, and sexual orientation/gender identity prejudice represent fear-based cognitive and behavioral patterns where the nervous system has categorized LGBTQ+ identities as sources of threat, moral violation, or existential danger requiring correction, rejection, or elimination. Individuals with these patterns experience anxiety when encountering sexual diversity, disgust responses to same-sex affection, catastrophic thinking about gender non-conformity, and defensive aggression masking deep fear. These patterns drive discrimination, violence, conversion attempts, and systemic oppression that traumatizes vulnerable populations.
The neurobiological mechanism involves early amygdala conditioning where sexual diversity became paired with threat through parental messaging, religious indoctrination, or peer group social threat. The insula becomes hyperactive to same-sex intimacy or gender non-conformity, generating disgust responses. The anterior cingulate becomes activated to perceived moral violation when encountering LGBTQ+ content. The amygdala's threat detection system has been hijacked to treat gender and sexual diversity as danger-level threat requiring protective action. In-group bias networks become hyperactive, creating us vs. them categorization where LGBTQ+ individuals are coded as existential threat to identity, family, or culture. The prefrontal cortex loses capacity for nuance, empathy, and rational assessment when sexual diversity triggers limbic threat response.
Our technique systematically deconditions the amygdala's threat associations with sexual orientation and gender diversity through targeted creative intervention. We identify the fear beliefs and in-group identity defenses that drive prejudicial patterns, then replace them with expanded capacity for human diversity and genuine compassion. Your nervous system shifts from threat-detection to recognition of shared humanity. Discriminatory impulses dissolve when the neural coding of LGBTQ+ people as threat is rewired. You access authentic moral frameworks, genuine religious faith beyond fear-based prejudice, cultural belonging through strength rather than exclusion, and liberated capacity for compassion.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Racism, Xenophobia, Ethnic & Racial Prejudice
This could be your breakthrough. Let's do this!
Your amygdala learned to perceive racial and ethnic otherness as tribal threat. The in-group bias system has gone haywire into violent tribal defense. Racism, xenophobia, and ethnic prejudice represent neurologically-encoded threat responses where populations of different racial, ethnic, or national origin have become coded as sources of danger, moral contamination, or existential threat to group survival. Individuals with activated prejudicial neural patterns experience automatic fear and suspicion of people from different racial or ethnic backgrounds, catastrophize threats they associate with outsiders, engage in discriminatory behavior ranging from avoidance to violence, and defend their prejudicial cognitions through defensive rationalization and conspiracy thinking.
The neurobiological mechanism involves ancient evolutionary in-group bias systems (tribal survival through group favoritism and out-group suspicion) that become hijacked by amygdala threat-conditioning in environments of scarcity, conflict, or cultural/political messaging linking racial/ethnic differences to danger. The amygdala automatically fires threat-detection when encountering racial/ethnic differences. The insula becomes activated to out-group populations, creating disgust and contamination avoidance. In-group bias networks (posterior cingulate, temporo-parietal region) generate intense in-group favoritism and out-group derogation. The prefrontal cortex loses capacity for nuance and empathy when threat-detection systems activate around racial/ethnic difference. Conspiracy beliefs and zero-sum thinking (their gain is our loss) become hardened neural patterns that prevent accurate threat assessment and mutual understanding.
Our technique targets the amygdala's threat-coding of racial and ethnic diversity and rebuilds the in-group/out-group balance through precision limbic recalibration. We dissolve fear-based threat associations and replace them with neural patterns of shared humanity and mutual benefit. The automatic prejudicial threat response dissolves when the amygdala's racial/ethnic threat-coding is rewired. You access restored capacity for racial justice, authentic respect for cultural diversity, genuine security that doesn't require othering, and freedom from the exhausting cognitive burden of prejudicial vigilance.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Misogyny, Gender-Based Violence & Fear of Women
This could be your breakthrough. Let's do this!
Your nervous system learned that female power, sexuality, and autonomy represent threat requiring control, diminishment, or elimination. The amygdala has been conditioned to perceive women as dangerous through socialization, trauma, or failed intimate bonds. Misogyny, gender-based violence, and the fear of female power represent psychological patterns where the nervous system codes female autonomy, sexuality, and authority as sources of existential threat requiring control, submission, humiliation, or violence. Individuals with activated misogynistic neural patterns experience intense anxiety around female authority, respond to female autonomy with defensive aggression, use sexual aggression or intimate violence to restore threatened dominance, engage in dehumanizing sexual objectification of women, and defend their hostile cognitions through elaborate rationalizations about female inferiority or dangerousness.
The neurobiological mechanism typically originates in early maternal experiences: maternal abandonment, rejection, or domination creates amygdala threat-conditioning around female presence, maternal control becomes encoded as existential threat, and the developing male nervous system never learns to trust female safety. Alternatively, experiences of female sexual rejection or perceived humiliation trigger amygdala threat responses that become generalized to all women. The insula becomes hypersensitive to female power and autonomy, generating disgust. The orbitofrontal cortex (responsible for reward evaluation) becomes dysregulated around female sexuality, causing sexual predation to feel rewarding. The lateral prefrontal cortex loses capacity for empathy toward female subjective experience. Testosterone-mediated aggression systems become sensitized to perceived female threat, creating hair-trigger reactivity. The nervous system becomes locked in a pattern where dominance over women feels like survival.
Our technique recalibrates the amygdala's threat-coding of female power through targeted creative reprogramming. We identify the early maternal/female threat associations and replace them with neural patterns of genuine safety with women. Your nervous system shifts from threat-response to authentic relational capacity. The automatic hostile/aggressive response to female authority and sexuality dissolves when deep trust with female presence is recoded. You access genuine intimate capacity, authentic sexuality, freedom from the depleting rage of misogyny, and the enrichment of genuine partnership with women as equals.
Related condition: For adolescent misogyny and gender-based violence patterns, this condition shares neurobiological mechanisms with Teen Bullying & Aggressive Defense.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Scapegoating, Hate Projection & Enemy Creation
This could be your breakthrough. Let's do this!
Your nervous system may have learned to discharge fear, shame, grievance, or powerlessness by locating a target to blame, punish, or cast out. Scapegoating and hate-projection are patterns in which diffuse internal distress or collective anxiety gets concentrated onto a person or group who becomes framed as the cause of decline, humiliation, impurity, or danger. Rather than tolerating uncertainty, grief, status loss, or complexity, the mind creates relief through simplification: if the enemy can be named, then pain appears explainable and aggression feels righteous. This mechanism can operate in families, workplaces, religious movements, politics, online culture, and mass movements.
The neurobiological mechanism involves threat-detection, projection, and social-bonding circuits becoming fused. The amygdala marks ambiguity, shame, and loss of control as danger, while the ventromedial prefrontal cortex constructs a blame narrative that relocates intolerable internal states onto an external target. The anterior insula can convert disgust, humiliation, or moral panic into visceral certainty that the target is contaminating or dangerous. Reward circuits then begin reinforcing outrage, group cohesion, and punishment fantasies because shared hatred produces belonging, certainty, and temporary relief from helplessness. The prefrontal cortex loses nuance as the nervous system becomes increasingly invested in enemy-construction over reality-testing.
Our technique targets the projection-and-threat circuitry that turns pain into persecution. We help the nervous system tolerate ambiguity, status injury, shame, and fear without needing a human target to carry them. This is not political persuasion or forced moral agreement. It is recalibration of the neural process that converts distress into hatred and belonging-through-exclusion. You experience reduced compulsion to blame, less attraction to enemy narratives, restored capacity for complexity and empathy, and a nervous system that no longer requires a scapegoat in order to feel organized or safe.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Tribalism, Groupthink & In-Group/Out-Group Bias (Us vs Them Syndrome)
This could be your breakthrough. Let's do this!
Your nervous system learned that group survival depends on unquestioning loyalty and viewing all outsiders as threat or competition. The amygdala has become hyperactive to any deviation from in-group consensus or any out-group contact. Tribalism, groupthink, and in-group/out-group bias represent neurologically-driven patterns where the brain becomes locked in zero-sum thinking (their gain is our loss) and loses capacity for independent thought, nuanced evaluation, or recognition of out-group humanity. Individuals with activated tribal neural patterns experience intense need to conform to group beliefs without question, experience anxiety when encountering out-group members or perspectives, respond to group dissent with aggression or rejection, engage in conspiratorial thinking that polarizes friends from enemies, and experience defensive rage when their tribal narratives are questioned.
The neurobiological mechanism involves hyperactivity of the amygdala's in-group bias circuits and threat-detection systems, combined with suppression of the prefrontal cortex's capacity for independent evaluation. The medial prefrontal cortex becomes specialized for in-group member processing while the temporoparietal region becomes active only for in-group preference. The anterior insula becomes oversensitized to out-group otherness, generating automatic disgust. The amygdala becomes hyperresponsive to threats to group identity, causing defensive aggression when group beliefs are questioned. The ventromedial prefrontal cortex loses capacity for weighing evidence impartially when tribal identity is activated. Reward circuits become sensitized to in-group affiliation and in-group dominance over out-groups, making tribal identity neurochemically addictive. In-group conformity becomes neurologically prioritized over truth-seeking and ethical reasoning.
Our technique recalibrates the amygdala's threat-response to out-group difference and restores prefrontal independence through targeted limbic intervention. We dissolve the neurochemical bonds that make tribal identity addictive and replace them with capacity for authentic values-driven thinking. Your nervous system shifts from tribal threat-detection to genuine problem-solving. The defensive rage and groupthink dissolve when the amygdala's polarized in-group/out-group coding is rewired toward genuine pluralism. You access independent thought, authentic values alignment, genuine security that doesn't require enemies, and freedom from the exhausting neurochemical addiction to tribal identity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Power, Aggression & Control
Power & Control Issues
This could be your breakthrough. Let's do this!
Your nervous system learned that maintaining control is necessary for survival. Power and dominance or compulsive control-seeking became how your nervous system manages threat. Power and control issues involve patterns of seeking control over others or situations, difficulty with loss of control, aggressive dominance-assertion, vulnerability-intolerance, and relational patterns where control becomes more important than connection. These create significant relationship damage and often restrict personal freedom through the exhausting effort to maintain control of uncontrollable systems.
The neurobiological mechanism often involves early experiences where the environment felt chaotic or threatening and control-seeking became the adaptive protective strategy. The amygdala became sensitized to perceived loss-of-control as existential threat. The ventromedial prefrontal cortex encodes control-seeking as a safety strategy. The empathy-processing systems may become downregulated when others' autonomy threatens felt sense of control. In cases of aggression-driven dominance, the orbitofrontal cortex becomes hyperactive in dominance-assessment and amygdala becomes reactive to perceived challenge. The nervous system learned that power resolves threat, though actual threat stems from vulnerability-intolerance rather than external danger.
Our technique recalibrates threat-perception around loss of control and restores capacity to tolerate appropriate vulnerability through targeted limbic intervention. We reduce amygdala reactivity to control-loss and increase tolerance for uncontrollable systems. Your nervous system regains capacity for genuine connection where autonomy need not threaten your sense of safety. You experience freedom from control-compulsion and restored capacity for healthy relationships and collaborative rather than dominance-based relating.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.IED - Rage and Intermittent Explosive Disorder
This could be your breakthrough. Let's do this!
Your nervous system is exploding because it never learned to breathe. That ends today. Intermittent Explosive Disorder and rage-related conditions are characterized by recurrent, sudden episodes of intense anger and aggressive behavior that are disproportionate to any provocation or stressor. Individuals experience these episodes as overwhelming and uncontrollable, often followed by remorse and distress about their behavior, particularly when loved ones have been harmed during the outburst. These rage episodes can devastate relationships, limit employment, and lead to legal consequences.
The neurobiological mechanism involves what researchers call a 'limbic hijack' where anxiety and high baseline stress trigger overwhelming amygdala activation that rapidly overwhelms the prefrontal cortex's ability to modulate response. This creates a self-reinforcing loop where the neurochemical 'rush' of anger and associated catecholamine release temporarily relieves the internal tension of chronic anxiety. The relief becomes reinforcing, leading to a cycle of compulsive rage outbursts where the individual becomes unconsciously driven to recreate that relief through anger. The nervous system has learned that rage is a more effective release mechanism than healthy self-regulation.
Our technique breaks this reinforcement cycle by providing more effective ways to downregulate the nervous system than the maladaptive pattern of rage. We reprogram the amygdala's threat detection and restore prefrontal regulation capacity. You access parasympathetic activation and calm presence instead of the rage cascade. This isn't anger management or talking about triggers. It's targeted recalibration of the nervous system's alarm and regulation systems. Rage episodes recede substantially, relationships heal, and you access genuine agency over your emotional responses.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Gun Addiction and Weapons Obsession
This could be your breakthrough. Let's do this!
Your nervous system learned that weapons represent power and control over threat. But that's a transaction with catastrophe. Gun addiction and compulsive weapons collection represent behavioral addiction to firearms and weapons acquisition, characterized by compulsive purchasing, obsessive focus on weapons capabilities, and escalating investment in firearms despite financial or relational consequences. Individuals with gun addiction often experience anxiety about vulnerability without weapons present, fear-based threat prediction, and a sense that accumulated weapons provide safety and control. However, research shows that gun access correlates with increased risk of harm to self, intimate partners, and children—the opposite of the safety promised by the nervous system's threat narrative.
The neurobiological mechanism involves a hijacking of the threat-response system where weapons become encoded as the solution to amygdala-driven threat perception. Anxiety drives the belief that weapons = safety, creating a compulsive acquisition pattern. The reward system becomes activated by weapons-acquisition as a way to manage existential threat-anxiety. Paradoxically, the presence of weapons amplifies threat-perception through increased responsibility-anxiety and hypervigilance. The amygdala becomes primed to detect threats that weapons must defend against, creating an escalating cycle of fear and acquisition. The nervous system essentially trades one threat (existential anxiety) for another (access to lethal means during moments of dysregulation).
Our technique recalibrates the threat-response system and restores genuine safety perception independent of weapons through targeted limbic intervention. We dissolve the false equivalence between weapons-access and actual safety. Your nervous system regains capacity to experience genuine security through nervous system regulation rather than external weapons. This isn't gun control advocacy or judgment. It's recoding of how your nervous system encodes threat and safety. You experience reduced anxiety-driven acquisition urges and restored sense of security.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Homicidal Ideation and Violent Urges
This could be your breakthrough. Let's do this!
Your amygdala is broadcasting violent solutions to threats that don't require violence. It's time to restore proportionate response capacity. Homicidal ideation refers to persistent, intrusive thoughts about harming or killing others, ranging from passive fantasies to active planning. Individuals experiencing homicidal ideation are often deeply distressed by their violent thoughts, which conflict with their values and desired identity. Homicidal ideation can emerge in psychiatric conditions (psychosis, severe personality disorders), in response to trauma or injustice, or in response to intense anger and threat-perception. When combined with impulsivity, access to weapons, or substance intoxication, homicidal ideation becomes a genuine public health risk. The individual is often trapped between despair about their violent thoughts and genuine danger of acting on them.
The neurobiological mechanism involves amygdala hyperactivity in response to perceived threat or injustice, combined with prefrontal cortex dysregulation that normally inhibits aggressive impulses. The anterior cingulate cortex becomes activated in error-detection mode, amplifying perception of threat or moral wrongdoing. The orbitofrontal cortex, which assesses threat-response proportionality, becomes dysregulated, leading to violent-response as seemingly proportionate to the perceived threat or injustice. In some cases, dopamine dysregulation creates reward-seeking through violent fantasy. The nervous system becomes trapped in a state where violent solutions seem necessary and justified.
Our technique recalibrates threat-response proportionality and restores prefrontal inhibition through targeted limbic intervention. We reduce amygdala-driven threat perception and restore accurate assessment of response options. Violent ideation recedes as the nervous system regains capacity for proportionate, non-violent responses to threat or injustice. This isn't judgment about the content of thoughts or coercion toward non-violence. It's recoding of how your nervous system generates response options to threat. You experience freedom from intrusive violent ideation and genuine security in non-violent capacity.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Opportunities for more emotional freedom
Paranoia and Scelerephobia - Fear of Strangers and Crime
This could be your breakthrough. Let's do this!
Your amygdala declared the world full of criminals and threats hidden in every stranger. It's time to restore accurate threat assessment. Paranoia is characterized by persistent, unjustified suspicion of others' intentions, belief that people are plotting against you, hypervigilance to threat signs, and often magical thinking about persecution. Scelerephobia (fear of criminals and crime) involves intense dread of being victimized by crime, avoidance of normal situations due to exaggerated crime risk, and hypervigilance to strangers. Together, these conditions create a state of perpetual threat perception where the social world feels hostile and dangerous, severely restricting social engagement and quality of life.
The neurobiological mechanism involves amygdala hyperactivity combined with failure of the prefrontal cortex to regulate threat interpretation and distinguish between genuine danger and neutral social cues. The amygdala becomes primed to detect threat in ambiguous social situations—a stranger's glance becomes evidence of malintent, accidental slights become intentional persecution. The insula becomes hyperactive, amplifying threat-related bodily sensations and creating the subjective experience of imminent danger. The theory of mind network—which interprets others' intentions—malfunctions, leading to systematic misinterpretation of benign intentions as harmful. The nervous system remains locked in a state of social threat hypervigilance.
Our technique recalibrates threat perception in social contexts and restores accurate threat-assessment through targeted limbic intervention. We dissolve the systematic bias toward threat interpretation and restore the amygdala's capacity to distinguish genuine danger from normal social situations. Paranoid ideation recedes as the nervous system regains accurate perception of others' intentions. This isn't cognitive therapy or social exposure. It's recoding of how your nervous system interprets social threat. You experience freedom from persecution beliefs and restored capacity for authentic social engagement.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Persecutor Role - Aggressive Control & Domination Pattern
This could be your breakthrough. Let's do this!
Your nervous system learned that the only way to maintain safety and control is through aggression, dominance, intimidation, and coercion, and that other people are threats that must be controlled or crushed. The Persecutor role in Karpman's Drama Triangle is characterized by someone who uses aggression, criticism, blame, control, intimidation, or violence to dominate others and maintain power. Unlike the narcissist's need for admiration or the antisocial person's lack of empathy, the persecutor's primary drive is control and dominance over others. They create fear and emotional injury in their relational circles, often leaving family members and partners in constant hypervigilance. The persecutor often unconsciously learned this pattern from their own early exposure to aggression, domination, or powerlessness-reversal trauma.
The neurobiological mechanism involves threat-detection circuits that are overactive in perceiving others as dangerous and requiring preemptive control. The amygdala generates persistent low-grade threat-response to others' autonomy or disagreement. The orbitofrontal cortex becomes hyperactive in reward-pathways connected to dominance and control, making aggression neurochemically rewarding. The ventromedial prefrontal cortex encodes a threat-based worldview ("Others will hurt me if I don't control them" or "Other people are obstacles to my needs"). The anterior insula becomes hyperactive in response to others' distress, but rather than generating empathy (as in healthy empathy), it generates satisfaction or justification ("They deserve it," "They needed to be controlled"). The dorsolateral prefrontal cortex may be hyperactive in strategic planning of control-tactics. Early trauma often involved either being violently controlled (leading to identification with the aggressor) or early powerlessness (leading to overcompensation through domination). In some cases, the persecutor is expressing unprocessed rage at historical injustices or powerlessness.
Our technique addresses the underlying threat-perception and powerlessness-dynamics that drive the persecutor pattern. We help the amygdala distinguish between genuine threat and perceived threats emerging from control-insecurity. We recalibrate the orbitofrontal cortex's hyper-rewarding of dominance and replace it with genuine reward from healthy power-sharing and relational reciprocity. We reprogram the ventromedial prefrontal cortex's threat-worldview. We help the anterior insula develop genuine empathy instead of satisfaction at others' pain. We address the early trauma that generated either identification with the aggressor or aggressive compensation for powerlessness. This work requires genuine motivation to change, as the persecutor often feels justified in their aggression. You experience reduction in aggressive impulses, capacity for relational power-sharing without experiencing powerlessness, genuine empathy for others' experience, freedom from the need to dominate, and the possibility of healthy relationships based on mutuality rather than dominance.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Teen Bullying & Aggressive Defense Mechanisms - Adolescent Peer Aggression
This could be your breakthrough. Let's do this!
Your adolescent is using aggression, dominance, and social cruelty as the primary way to manage a terrified, shame-filled nervous system. Teen bullying and aggressive defense occur when an adolescent (whether as perpetrator or in reactive aggression) uses social cruelty, physical aggression, or dominance-establishment as the default response to threat, rejection, powerlessness, or shame. The bullying adolescent may be working compulsively to establish and defend status-position in the peer hierarchy, to channel rage from family trauma into peer-directed targets, to manage deep shame through shame-projection, or to access the status-dopamine reward of dominance. Bullying behavior can be entrenched across multiple peer contexts, can escalate toward violence, and generates profound social consequences and isolation even as it provides temporary status-reward. The aggression is often neurologically automatic—shame-activation → amygdala threat-response → aggression-response without prefrontal evaluation.
The neurobiological mechanism: the amygdala has become sensitized to threat and shame-detection, and the default response-pathway is aggression. The orbitalfrontal cortex (social hierarchy processing) has become locked into dominance-seeking as the primary solution to status-anxiety. The ventromedial prefrontal cortex encodes aggression as the appropriate response to threat/shame. The anterior insula becomes hyperresponsive to signs of peer rejection or status-lowering, triggering protective aggression. Dopamine-reward has become linked to dominance and peer-fear of the adolescent. The dorsolateral prefrontal cortex loses capacity for empathy and social-information processing when status-threat is activated. Beneath the aggression is typically profound shame, fear of rejection, or family-learned violence-as-coping.
Our technique decouples shame-activation from aggression-response and addresses the underlying terror/shame that the aggression protects. We help the adolescent's orbitalfrontal cortex distinguish between genuine status-threat and perceived status-threat, and develop alternative status-pathways that don't depend on aggression. The amygdala becomes less reactive to status-challenge situations. The ventromedial prefrontal cortex develops new values around genuine peer connection rather than fear-based dominance. The anterior insula recalibrates to detect genuine threat vs. social discomfort. The adolescent develops capacity for authentic peer relationships based on reciprocal respect rather than fear and dominance, decreased aggression and bullying, and integration of shame experiences rather than projection onto others.
This could be your breakthrough. Let's do this! Sign up now.
Disclaimer:
This study is conducted for neuroscience research purposes and does not constitute medical treatment, psychological counseling, or clinical therapy. The researcher is a student of neuroscience and is not a licensed medical doctor or psychologist. All procedures are strictly for investigative data collection; therefore, participants should not interpret any part of this interaction as medical advice or a substitute for professional healthcare.Partners & Pioneers
For decades, neuroscientists have puzzled over why our brains react to perceived threats in ways that feel beyond conscious control. In the 1990s, Paul MacLean and later Daniel Goleman introduced the concept of "amygdala hijacks" - moments when emotion overwhelms reason. Their work showed that trauma and anxiety stem from a limbic loop, a self-reinforcing circuit where emotional memory hardens into fixed neural patterns. For years, these patterns seemed unchangeable in adults. But recent neuroplasticity research reveals something remarkable: these hardened loops can be reopened, rewired, and healed. This has transformed how we treat anxiety, PTSD, phobias, and other neurological conditions.
Our research is built on the pioneering work of world-class scientists whose discoveries have advanced our understanding of neuroplasticity, limbic loops, and the therapeutic potential of targeting these pathways to reduce neurological symptoms.
We are deeply grateful for their contributions to science and humanity.

Eric Kandel
University Professor, Nobel Laureate
Columbia University
Department of Neuroscience
Research Focus
Physiological Basis of Memory Storage
Research
Eric Kandel's Nobel Prize winning research on the physiological basis of memory storage provides one of the deepest foundations for NeuroRecursion: experience becomes durable when neural activity changes synaptic strength. His work established that memory is not an abstract psychological phenomenon floating above biology, but a physical process embedded in neurons and altered by learning. That insight is indispensable for any attempt to rewrite hardened fear and trauma patterns.
Kandel demonstrated that synaptic plasticity allows experience to be converted into long-term change through identifiable cellular and molecular mechanisms. This matters directly for NeuroRecursion because the intervention assumes that emotionally charged experiences can be re-encoded rather than merely suppressed. If fear memories are stored through modifiable synaptic processes, then the limbic system's threat associations are not fixed destiny; they are biological patterns capable of revision.
Kandel's work also created the modern bridge between molecular memory science and clinical disorders such as PTSD and neurodegeneration. NeuroRecursion sits downstream of that bridge: it depends on the premise that intense, targeted experience can alter the structure of remembered threat. Kandel supplied the canonical proof that memory is stored in living, changing synapses and therefore can, under the right conditions, be fundamentally rewritten.
Research Areas
Susumu Tonegawa
Professor, Nobel Laureate
Massachusetts Institute of Technology
Department of Biology and Neuroscience
Research Focus
Engram Cells and Memory Circuitry
Research
Susumu Tonegawa's neuroscience work on engram cells brought extraordinary precision to the study of memory by identifying physical traces of stored experience in the brain. His research shows that memories are not vague psychological impressions but can be localized, reactivated, and experimentally manipulated within specific neural populations. That level of specificity is profoundly relevant to NeuroRecursion's ambition to alter hardened trauma-related memory structures.
By tracing memory engrams in the hippocampus and related systems, Tonegawa helped establish that recall and emotional valence can be modified through targeted reactivation. This has major implications for retrograde amnesia, dementia, and fear memory research, but it also speaks directly to therapeutic rewriting: if memory traces can be accessed and shifted, the original emotional meaning of an experience is not neurologically untouchable. NeuroRecursion operates on the same assumption at a psychological scale.
Tonegawa's work provides a mechanistic bridge between memory science and intervention. Rather than treating memory as a static archive, his research presents it as a living circuit process subject to updating under the right conditions. That scientific picture strengthens the plausibility of any method, including NeuroRecursion, that seeks to reactivate deeply encoded fear and then transform its downstream significance.
Research Areas
Ann Graybiel
Institute Professor
MIT McGovern Institute for Brain Research
Department of Brain and Cognitive Sciences
Education
B.S. University of Illinois, Ph.D. University of Wisconsin
Research Focus
Neural Basis of Habit and Reward
Research
Ann Graybiel's research on habit loops directly parallels NeuroRecursion's target: hardened neural patterns that feel involuntary and resist rational override. Her discovery that habits become encoded in specific basal ganglia circuits—and can be triggered by environmental cues independent of deliberate intention—maps exactly onto how traumatic fear responses operate: as automatic, stimulus-driven patterns stored in neural circuits that exist outside conscious control.
Graybiel's crucial insight is that habit loops can be interrupted and rewritten, but the method is not simple suppression. Her work reveals that the neural pathways encoding habits are modifiable, though the modification requires more than willpower—it requires understanding the circuit's logic and engaging it directly. NeuroRecursion applies this principle to fear and trauma loops: by inundating the limbic system with massive quantities of trauma-relevant scenarios, it forces the circuit to process millions of comparisons, ultimately degrading the original association between trigger and threat response.
Graybiel's mapping of the neural basis of stuck repetitive behaviors validates NeuroRecursion's assumption that these patterns—anxiety, fear, compulsive responses—are not permanent features of the self but rewirable neural circuits that can be restructured through sufficiently powerful interventions that engage the circuits' own processing mechanisms.
Research Areas

Carla Shatz
Professor of Biology and Neurobiology
Stanford University
Department of Biology
Education
B.S. Cornell University, Ph.D. UC Berkeley
Research Focus
Developmental Neuroscience and Neural Plasticity
Research
Carla Shatz's discovery of activity-dependent competition in neural development reveals the cellular mechanism underlying NeuroRecursion's efficacy: synapses are continuously evaluated, strengthened or weakened based on patterns of neural activity. This principle extends far beyond development—it indicates that throughout life, the brain refines connections based on what it experiences.
Shatz's work on critical periods demonstrates that heightened plasticity creates windows of enhanced malleability, a principle NeuroRecursion harnesses. By overwhelming the limbic system with millions of high-valence recursive comparisons, NeuroRecursion functionally creates an episode of heightened plasticity where threat circuits become susceptible to modification. The intense, saturation-level activity Shatz's research suggests will preferentially strengthen new associations over old ones.
Her evidence that neural connections are continuously evaluated and refined based on activity patterns validates NeuroRecursion's core mechanism: if the limbic system is presented with massive quantities of survival-relevant data (the recursive traumatic scenarios) that contradict the original threat association, activity-dependent plasticity will preferentially strengthen the new, safety-based associations while degrading the original pathological circuit. Shatz's synaptic-level insights explain how intensive, targeted neural activity can fundamentally restructure even long-standing fear circuits.
Research Areas

Karl Friston
Neuroscientist, Free-Energy Principle Pioneer
UCL Institute of Neurology, University College London
Department of Wellcome Centre for Neuroimaging
Education
B.Sc. University of London, Ph.D. University of London
Research Focus
Theoretical Neuroscience and Brain Dynamics
Research
NeuroRecursion works using Karl Friston's free-energy principle. His theory that the brain constantly generates threat predictions and updates them when violated by actual experience reveals how NeuroRecursion works subconsciously at the deepest computational level.
Friston's insight that the brain is fundamentally a prediction machine whose goal is minimizing prediction error illuminates the core of NeuroRecursion's mechanism. The hardened limbic loop exists because the brain has encoded a strong threat prediction about a stimulus that, in the person's current reality, no longer represents actual threat. By generating millions of recursive threat scenarios that violate the original threat prediction, NeuroRecursion creates cascading prediction errors so massive that the brain's threat model must be fundamentally updated.
NeuroRecursion implements Friston's principle at clinical scale: by overwhelming the limbic system's threat-prediction machinery with such enormous quantities of contradictory, high-valence information that the brain's Bayesian inference engine can no longer maintain its original threat prediction, NeuroRecursion forces a global update of threat models. The neutralization event—where the original trigger is no longer recognized as threat—represents the massive prediction error cascade triggering fundamental revision of the brain's threat posterior distribution, precisely as Friston's theory predicts.
Research Areas

Paul MacLean
Neuroscientist, Brain Evolution Researcher
National Institute of Mental Health (NIMH)
Department of Laboratory of Brain Evolution and Behavior
Education
B.S. Columbia University, M.D. Yale University
Research Focus
Brain Evolution and Emotional Systems
Research
Paul MacLean's triune brain model provides the foundational concept for NeuroRecursion: the limbic system as a hardened, ancient survival mechanism that can be accessed and restructured through neocortical intervention. His mapping of the limbic system revealed how the amygdala, hippocampus, and related structures encode threat-based emotional memories in ways that bypass rational thought—the very neural organization that NeuroRecursion targets.
MacLean's insight that the limbic system is not subordinate to reason but rather a dominant organizing principle illuminates why direct willpower fails to change hardened emotional loops. His work establishes that the limbic system operates according to its own logic, one where fear and survival responses are encoded in persistent neural circuits. NeuroRecursion's approach of bypassing rational suppression and instead flooding the limbic system with high-valence recursive scenarios works precisely because it speaks in the limbic system's native language of comparison, hierarchy, and survival threat.
By mapping the structure MacLean identified, NeuroRecursion restructures limbic circuits through the prefrontal cortex's narrative architecture, converting MacLean's understanding of limbic dominance into a therapeutic mechanism for its transformation.
Research Areas
Joseph LeDoux
Professor of Neural Science
New York University
Department of Neural Science
Research Focus
Amygdala Circuits and Fear Learning
Research
Joseph LeDoux redefined modern understanding of the amygdala by showing how threat processing and fear conditioning are implemented in specific neural circuits rather than vague emotional abstractions. His work made fear scientifically tractable: something that can be mapped, tested, and altered at the level of circuitry. That makes him one of the most directly relevant pioneers for any model centered on limbic threat loops.
LeDoux's research bridges the limbic system's hardware with the lived clinical realities of anxiety, phobias, and trauma. He demonstrated how sensory information can rapidly trigger defensive responses through amygdala pathways before reflective reasoning fully engages. NeuroRecursion is aimed precisely at this problem: automatic fear predictions that outrun conscious logic and continue firing even when the original danger is gone.
By identifying the neural pathways through which fear is learned and expressed, LeDoux provided a circuit-level map for therapeutic intervention. NeuroRecursion builds on the same premise that fear is not a mystical essence but a trainable output of organized systems. His work validates the idea that if the threat circuits of the amygdala can be taught a trigger no longer predicts danger, the emotional response can be transformed at the source rather than merely managed on the surface.
Research Areas

Trevor Robbins
Professor of Cognitive Neuroscience
University of Cambridge
Department of Psychology
Education
B.A. Oxford University, Ph.D. Cambridge University
Research Focus
Cognitive Neuroscience and Behavioral Control
Research
Trevor Robbins's research on prefrontal-limbic circuits directly maps NeuroRecursion's architecture: the prefrontal cortex as a narrative architect that can override, reorganize, and integrate limbic survival responses. His work identifying the specific circuits that govern impulse control and emotional regulation reveals the neural substrate through which NeuroRecursion operates.
Robbins's fundamental insight—that dysregulation in prefrontal-limbic communication underlies fear, anxiety, and compulsive behaviors—frames the problem NeuroRecursion solves. His evidence that these circuits can be rebalanced through targeted intervention validates NeuroRecursion's core assumption: by leveraging the prefrontal cortex's narrative architecture to construct and process absurd, high-valence traumatic scenarios, one can restructure the limbic system's threat database and rebalance its relationship to prefrontal governance.
NeuroRecursion implements Robbins's circuit-level understanding at a metacognitive scale: rather than using pharmacological or simple behavioral interventions, it employs the prefrontal cortex's unique capability for imagination and narrative construction to generate recursive scenarios that so thoroughly challenge the limbic system's threat assumptions that the original trigger is no longer recognized as a biologically relevant threat—effectively rebalancing the prefrontal-limbic relationship at the deepest level.
Research Areas
Elizabeth Phelps
Pershing Square Professor of Human Evolutionary Biology
Harvard University
Department of Human Evolutionary Biology
Research Focus
Emotion, Memory, and Human Decision-Making
Research
Elizabeth Phelps is a leading figure in cognitive neuroscience whose work has clarified how emotion and memory interact in the human brain. She has mapped the relationship between the amygdala and cortical systems in shaping social behavior, valuation, and decision-making. For NeuroRecursion, her importance lies in showing that emotional salience and memory are not separable processes but part of a tightly integrated architecture that determines how people interpret risk and act under uncertainty.
Phelps's research helps translate fear and emotional learning from animal models into human neuroscience. She has shown how human amygdala-cortex interactions guide attention, bias memory, and influence choices in social and uncertain environments. NeuroRecursion depends on exactly this kind of interaction: a top-down narrative system engaging and ultimately re-educating bottom-up emotional predictions.
Her work also supports the idea that changing emotional memory changes future judgment, not just present distress. When the significance of a remembered threat is altered, the person's social behavior and decision-making can shift with it. Phelps therefore provides a human-level bridge between laboratory emotion science and the practical ambition of therapeutic rewiring.
Research Areas

Takao Hensch
Professor of Molecular and Cellular Biology
Harvard University
Department of Molecular and Cellular Biology
Research Focus
Critical Period Biology and Reopened Plasticity
Research
Takao Hensch is recognized for identifying critical periods in brain development and the biological mechanisms that open and close these windows of heightened plasticity. His work showed that the brain's capacity for rapid reorganization is actively gated by identifiable molecular and circuit conditions. This is directly relevant to NeuroRecursion because the intervention presumes that even apparently closed adult threat loops can be pushed back into a state of malleability.
Hensch's research on restoring plasticity after developmental windows have narrowed has important implications for conditions such as autism and amblyopia, but its significance is broader: it demonstrates that plasticity is not an all-or-nothing childhood event. Instead, it is a regulated state that can potentially be re-engaged. NeuroRecursion's intensive recursive scenarios can be understood within that same ambition: creating the conditions under which entrenched emotional circuitry becomes writable again.
By identifying the biological triggers that regulate sensitive periods, Hensch helped move neuroplasticity from metaphor to mechanism. NeuroRecursion benefits from that shift because it frames limbic rewiring as a problem of reopening change-capacity, not merely adding insight. His work supports the idea that therapeutic transformation may require more than persuasion; it may require re-establishing the neural conditions under which deep updating becomes possible.
Research Areas

Erin Schuman
Director
Max Planck Institute for Brain Research
Department of Synaptic Systems and Plasticity
Education
B.S. University of Michigan, Ph.D. UC San Diego
Research Focus
Molecular Basis of Synaptic Plasticity
Research
Erin Schuman's discovery of molecular machinery for synaptic remodeling reveals the cellular basis for how NeuroRecursion's effects become permanent: memory reconsolidation operates through precisely the molecular mechanisms Schuman studies. During the reconsolidation window—the labile period after memory reactivation—new patterns of neural activity reshape synaptic strength through local protein synthesis.
Schuman's work showing that synaptic strength is dynamically regulated by activity-dependent molecular signals explains the mechanism by which NeuroRecursion's recursive scenarios produce lasting change. As the limbic system processes millions of high-valence comparative scenarios, the activity triggered by these novel threat paradigms recruits local protein synthesis to strengthen new, safety-based synaptic connections while allowing original fear circuits to weaken through disuse.
Schuman's evidence that neurons possess exquisite molecular machinery for precisely restructuring synaptic connections in response to specific patterns of activity validates NeuroRecursion's assumption that sufficient, well-targeted neural activity can fundamentally rewrite even deeply embedded fear memories. Her work at the molecular level demonstrates that the brain is equipped to translate the massive prediction errors generated by NeuroRecursion's recursive scenarios into permanent structural changes—converting limbic loops into permanently modified circuits.
Research Areas

Michael Merzenich
Professor Emeritus
University of California, San Francisco
Department of Neuroscience
Research Focus
Adult Neuroplasticity and Cortical Reorganization
Research
Michael Merzenich is one of the principal pioneers of adult brain plasticity, showing that the mature brain retains the capacity to reorganize itself in response to training, injury, and altered experience. His work directly challenges the old assumption that major rewiring belongs only to childhood. For NeuroRecursion, that is not a side note but a prerequisite: if adult brains cannot change deeply, the whole therapeutic project collapses.
Merzenich demonstrated that neural maps in the adult cortex can be refined and reorganized through intensive, targeted engagement. This principle has shaped neurological rehabilitation, sensory retraining, and treatment approaches for disorders involving maladaptive processing. NeuroRecursion relies on the same underlying logic, though applied to emotional-threat networks rather than primary sensory maps: repeated, strategically structured experience can drive lasting circuit change.
His work is especially important because it grounds plasticity in disciplined neuroscience rather than inspirational metaphor. NeuroRecursion's claim that entrenched fear patterns can be destabilized and replaced becomes far more credible in the context of Merzenich's evidence that the adult nervous system is continuously trainable. He made plasticity a mainstream biological fact, and that fact underwrites any serious attempt to therapeutically rewire the limbic system.
Research Areas

Lisa Feldman Barrett
University Distinguished Professor
Northeastern University
Department of Psychology
Research Focus
Constructed Emotion and Predictive Affective Neuroscience
Research
Lisa Feldman Barrett's theory of constructed emotion challenges the classical view that the brain contains fixed, fingerprint-like emotional programs waiting to be triggered. Instead, she argues that the brain predicts and constructs emotional experience from past learning, bodily signals, and context. This is highly relevant to NeuroRecursion because it reframes fear and distress as model-based predictions rather than permanent essences embedded in the self.
Barrett's work suggests that the limbic system does not merely emit preset emotions, but participates in predictive processes that assemble meaning from prior experience. That perspective aligns naturally with therapeutic approaches that seek to change emotional life by changing what the brain expects, categorizes, and interprets. NeuroRecursion similarly assumes that if the brain's threat predictions are overwhelmed and revised, the resulting emotional outputs can change dramatically.
Her research broadens the scientific basis for treating affective disorders by showing that emotional suffering may be altered through prediction, categorization, and interoceptive recalibration. NeuroRecursion can be understood as an extreme intervention into that predictive machinery: a method for forcing the brain to generate new inferences about danger, safety, and meaning. Barrett helps make clear why changing past-conditioned interpretation can change lived emotion itself.
Research Areas
Gül Dölen
Professor, Researcher, and Neuroscientist
Berkeley Neuroscience Institute, University of California, Berkeley
Department of Psychology
Education
MD/PhD Brown University/Massachusetts Institute of Technology
Research Focus
Behavioral and Systems Neuroscience
Research
Gül Dölen's work on reopening critical periods of neural plasticity in adults directly addresses a central challenge in NeuroRecursion: how to make a hardened, adult limbic system malleable again. Her discoveries that psychedelics and other interventions can dissolve the structural barriers to plasticity provide proof-of-concept that adult neural reorganization is possible, even for circuits that seem permanently fixed.
Dölen's research reveals that the extracellular matrix—physical scaffolding surrounding synapses—gates when and whether the brain can rewire itself. This molecular mechanism explains why direct psychological approaches often fail on deeply encoded, long-standing threat memories: the neural architecture itself has hardened. NeuroRecursion's intensive recursive scenarios operate in a similar vein: by creating such extreme prediction mismatch that the brain's threat-detection system is fundamentally destabilized, NeuroRecursion may create a state of heightened plasticity where the limbic system becomes amenable to rewriting.
Dölen's evidence that core aspects of brain reorganization can be triggered without pharmacological intervention—that the brain responds to contextual factors and extraordinary cognitive challenge—suggests that the recursive, high-valence challenge of NeuroRecursion scenarios could itself trigger the reopening of plasticity windows needed for limbic loop restructuring. Her work validates the possibility that adult trauma circuits, seemingly immutable, can be fundamentally rewired through properly targeted intervention.
Research Areas

Karim Nader
Professor of Psychology
McGill University
Department of Psychology
Education
B.S. McGill University, Ph.D. Hebrew University
Research Focus
Mechanisms of Memory Consolidation and Reconsolidation
Research
Karim Nader's discovery of memory reconsolidation provides the terminal mechanism for NeuroRecursion: his finding that traumatic memories become labile and modifiable during reactivation explains how the limbic system's hardened loops can be permanently restructured. NeuroRecursion does not simply suppress fear—it leverages Nader's reconsolidation window to fundamentally rewrite the original memory trace.
Nader's work revealed that when a threat memory is reactivated, it enters a window of instability where it can be updated with new information before being reconsolidated. NeuroRecursion exploits this window by forcing the limbic system to reactivate the original trauma memory repeatedly while overwhelmingly exposing it to survival-relevant scenarios that contradict the original threat association.
Nader's elegant insight explains NeuroRecursion's specific structure: the prefrontal cortex as narrative architect doesn't simply generate threat scenarios; it generates thousands of absurd, wildly elaborate trauma scenarios across the five Fs—saturating the threat-memory system with so much contradictory information during the reconsolidation window that the original fear memory is fundamentally updated. The neutralization event occurs when the reconsolidated memory no longer encodes the original trigger as a threat, permanence achieved through Nader's molecular mechanism of memory modification.
Research Areas

Daniela Schiller
Associate Professor of Psychiatry and Neuroscience
Icahn School of Medicine at Mount Sinai
Department of Psychiatry and Neuroscience
Education
B.S. Tel Aviv University, Ph.D. Hebrew University
Research Focus
Memory Reconsolidation and Fear Extinction
Research
Daniela Schiller's landmark research provides the clinical proof-of-concept that NeuroRecursion aims to achieve: permanent fear neutralization through reconsolidation-based memory updating. Her demonstration that fear extinction can be rendered permanent—lasting weeks and months—rather than temporary shows that the terminal neutralization event NeuroRecursion targets is scientifically achievable.
Schiller's critical insight is that reconsolidation-based updating produces qualitatively different outcomes from surface extinction: it doesn't leave the original fear memory intact alongside a new non-fear memory, but rather fundamentally modifies the original memory itself. NeuroRecursion operates precisely at this level—not teaching the limbic system that the trigger is safe (which could be forgotten or overcome by stress), but rewriting the original memory so that the trigger is no longer encoded as a threat signal.
Schiller's evidence that fear prevention is possible by intervening at the reconsolidation level validates NeuroRecursion's entire strategy. Her work demonstrates that the neutralization event—where the limbic system no longer recognizes the original trigger as biologically relevant—is not a therapeutic fantasy but an achievable outcome through properly targeted intervention. Her research shows that the "absence of fear" NeuroRecursion aims for is not suppression or habituation but genuine, permanent modification of the threat memory itself, preventing the return of fear that so often characterizes traditional exposure therapies.
Research Areas

Michael Meaney
Professor
McGill University
Department of Psychiatry
Research Focus
Epigenetics of Stress and Early Experience
Research
Michael Meaney's research on the epigenetics of stress revealed how early experience can become biologically embedded in the brain. His work showed that maternal care and early-life stress alter gene expression in limbic structures such as the hippocampus, producing lasting differences in stress regulation and vulnerability. This gives NeuroRecursion an important developmental context: threat sensitivity is not only learned psychologically, but sculpted into the body's regulatory architecture.
Meaney demonstrated that the quality of early caregiving changes how the brain and endocrine system respond to future adversity. That insight is crucial for understanding why some individuals become highly vulnerable to depression, anxiety, or trauma-related dysregulation. NeuroRecursion addresses the downstream consequences of that vulnerability by attempting to rewrite the threat patterns the nervous system has encoded, but Meaney helps explain how those patterns were made so durable in the first place.
His work also matters because it breaks the false opposition between biology and life history. Experience changes biology; biology then shapes future experience. NeuroRecursion depends on the same core principle, though applied therapeutically rather than developmentally: sufficiently powerful experience can change the operating logic of the nervous system. Meaney's work validates the idea that emotional suffering can be rooted in plastic, modifiable biological systems rather than fixed defects.
Research Areas

Bo Li
Professor at the School of Life Sciences
Tsinghua University
Department of Neural Circuits and Behavior
Education
B.S. Tsinghua University, Ph.D. UC Berkeley
Research Focus
Neural Circuits of Emotion and Social Behavior
Research
Bo Li's mapping of fear circuits and the neural basis of threat-driven emotional hierarchies reveals the exact target NeuroRecursion aims to restructure: the specific neural populations that generate automatic fear responses to originally traumatic triggers. His work showing that fear and aggression are not monolithic but rather organized in distinct, modifiable circuits validates NeuroRecursion's assumption that fear can be parsed, weakened, and ultimately neutralized through circuit-level intervention.
Li's insight that emotional responses emerge from definable neural populations demonstrates that fear is not a global, irreversible state but rather an output of specific circuits that process threat comparisons. NeuroRecursion operates at precisely this level: by flooding Li's fear circuits with millions of recursive threat scenarios, it changes the information these circuits process and the comparative judgments they make about threat relevance.
Li's evidence that emotional responses can be precisely targeted through understanding their circuit organization validates NeuroRecursion's core strategy: identifying the hardened limbic loops that generate fear responses and overwhelming them with new survival-relevant data that ultimately convinces the neural populations driving fear that the original trigger no longer represents a biologically relevant threat. His circuit-level mapping reveals how NeuroRecursion achieves its terminal neutralization event.
Research Areas

Daniel M. Wegner
Professor of Psychology
Harvard University
Department of Psychology
Education
B.A. Duke University, Ph.D. Duke University
Research Focus
Psychology of Mental Control and Self-Regulation
Research
Daniel Wegner's "ironic process" is the exponential mechanism that drives the subconscious through millions of recursive comparisons. His discovery that suppression paradoxically strengthens unwanted thoughts explains why traditional anxiety management—"don't think about the threat"—fails and why NeuroRecursion employs the opposite strategy: overwhelming engagement with the threat rather than avoidance.
Wegner's insights into how direct mental control can backfire reveal the trap hardened limbic loops have created. The more a trauma survivor tries not to think about their trigger, the stronger the anxious preoccupation becomes. NeuroRecursion inverts this dynamic: instead of suppressing the threat memory, it employs the ironic process to force exhaustive engagement with the threat—saturation of the Bayesian inference engine with millions of high-valence scenarios that ultimately overwhelm the original traumatic association.
Wegner's theory explains NeuroRecursion's counter-intuitive methodology: by forcing the subconscious to process an overwhelming flood of threat information (rather than suppressing it), the ironic process is harnessed to produce the opposite of its typical effect. The saturation prevents the fixation that suppression creates, instead producing neutralization through exhaustion of the threat-comparison capacity. Wegner's work validates NeuroRecursion's core strategic insight: working with the mind's mechanisms rather than against them.
Research Areas
Daniel Goleman
Psychologist, Science Journalist, Author
Contributor to Psychology Today, Science Times
Department of Psychology and Neuroscience
Education
B.A. Amherst College, Ph.D. Harvard University
Research Focus
Emotional Intelligence and Social-Emotional Learning
Research
Daniel Goleman's concept of the "amygdala hijack" names the exact problem NeuroRecursion solves: the rapid, pre-conscious triggering of limbic threat responses that overwhelm prefrontal control. His popularization revealed why traditional cognitive approaches fail—the amygdala doesn't wait for rational persuasion; it acts on ancient survival rules encoded in memory.
Goleman's work established that emotional patterns, though powerful, are not fixed destinies but modifiable neural responses. This recognition is foundational to NeuroRecursion's hypothesis: if amygdala hijacks can be triggered automatically, they can also be un-learned, re-mapped, and neutralized through targeted intervention. His work frames the problem in neural terms that make therapeutic transformation conceivable.
NeuroRecursion extends Goleman's insight by offering a specific mechanism: rather than trying to strengthen rational impulse control (which amygdala hijacks bypass), it employs high-valence recursive scenarios that overwhelm the limbic system's threat database, forcing millions of comparison computations that ultimately convince the amygdala that the original trigger is no longer a biologically relevant threat—achieving the neutralization Goleman suggested was possible through understanding emotion's neural basis.
Research Areas

Mary Galea
Professorial Fellow at the Department of Medicine
University of Melbourne
Department of Neuroscience
Education
B.S. University of Melbourne, Ph.D. University of Melbourne
Research Focus
Neuroplasticity and Motor Rehabilitation
Research
Mary Galea's research demonstrating that the adult brain retains remarkable capacity for reorganization in response to intensive experience directly validates NeuroRecursion's core assumption: that even deeply established trauma circuits can be restructured through sufficiently targeted, activity-dependent plasticity. Her work dispels the myth that adult brains are fixed, showing that organized, intensive engagement can induce measurable neural reorganization even in mature neural tissue.
Galea's evidence that activity-dependent plasticity can be systematically engaged through targeted, high-intensity intervention mirrors NeuroRecursion's strategy precisely. Just as rehabilitation induces motor cortex reorganization through intensive, specific motor practice, NeuroRecursion induces limbic reorganization through intensive, specific emotional-threat practice—the recursive scenarios weighted with the five Fs of survival response.
Galea's demonstration that recovery is possible through mechanisms of activity-dependent plasticity that can be deliberately actuated provides crucial validation that NeuroRecursion's intensive approach is not merely theoretical but grounded in demonstrated principles of adult neural reorganization. Her work extends the neurorehabilitation model to emotional and limbic domains, showing that the same principles producing motor recovery can produce emotional/limbic recovery through sufficiently intense, intentional engagement of the circuits requiring modification.
Research Areas
Giacomo Indiveri
Professor at the Institute for Neuroinformatics
ETH Zurich
Department of Neuromorphic Engineering
Education
B.S. University of Genoa, Ph.D. University of Genoa
Research Focus
Neuromorphic Engineering and Learning Systems
Research
Giacomo Indiveri's neuromorphic systems provide a computational model for understanding how the limbic system operates as a survival inference engine. His work showing that learning and adaptation can emerge from local circuits without centralized control mirrors the limbic system's decentralized threat-detection architecture—networks of amygdala, hippocampus, and related structures that process threat information through local comparisons rather than centralized reasoning.
Indiveri's research reveals how analog neural circuits—like the limbic system—process continuous, weighted information streams to make rapid responses. This computational perspective illuminates why the limbic system can be so difficult to override with rational argument: it operates according to principles of local circuit computation that don't depend on centralized conscious control.
However, NeuroRecursion's approach works not by disrupting the limbic system's local computation, but by flooding it with overwhelming quantities of new comparative data. Indiveri's insight that neural systems achieve flexibility through responsiveness to changing environments suggests that if the limbic system's threat-comparison circuits are exposed to sufficient new data—millions of recursive scenarios that violate threat predictions—they will reorganize around the new information, fundamentally altering threat associations without requiring centralized rational override.
Research Areas
Yukiyasu Kamitani
Professor at the Graduate School of Informatics
University of Tokyo
Department of Computational Neuroscience
Education
B.S. University of Tokyo, Ph.D. University of Tokyo
Research Focus
Computational Neuroscience and Brain Decoding
Research
Yukiyasu Kamitani's brain decoding research provides tools for monitoring NeuroRecursion's neural mechanism: tracking whether interventions shift the balance of dominance from limbic to prefrontal processing. His ability to decode neural states and internal imagery offers a method for understanding the neural signatures of NeuroRecursion's core transformation: the shift from limbic-driven fear reactivity to prefrontal-integrated narrative processing.
Kamitani's work on the brain's generative capacity—its ability to construct and sustain internal models—is foundational to NeuroRecursion's method. The intervention relies on the prefrontal cortex's unique capacity for imagination and narrative construction: the generation of synthetic, high-valence traumatic scenarios that overwhelm the limbic system's threat database. Kamitani's research validates that this imaginative capacity is not superficial but capable of generating neural states as powerful as real-world threats.
Kamitani's discoveries that brain activity can be decoded and neural patterns can be influenced provide emerging tools for understanding and optimizing NeuroRecursion's mechanism. His research suggests that by generating internally imagined scenarios of sufficient vividness and emotional valence, one can create limbic system activation patterns comparable to actual threat exposure—enabling the reconsolidation-based restructuring that forms NeuroRecursion's core mechanism.
Research Areas
Aditya Murthy
Professor at the Centre for Neuroscience
Indian Institute of Science (IISc) Bangalore
Department of Neuroscience
Education
B.Tech Indian Institute of Technology, Ph.D. Johns Hopkins University
Research Focus
Motor Neuroscience and Learning
Research
Aditya Murthy's research on motor learning and neural reorganization provides a model for how NeuroRecursion restructures emotional circuits. His work showing that practice and repeated activity reshape neural networks across multiple brain systems—cerebellum, cortex, basal ganglia—demonstrates that intensive, targeted repetition produces measurable circuit reorganization.
Murthy's evidence that motor learning involves dynamic reorganization of entire networks rather than isolated circuits parallels NeuroRecursion's mechanism: the recursive scenarios do not simply suppress fear but reorganize entire fear networks by forcing thousands of iterations of threat comparison and resolution. The repeated, high-valence processing demands of NeuroRecursion mirror motor learning's principle that intensive practice produces neural reorganization.
Murthy's insight that the nervous system continuously refines performance through active reorganization suggests that NeuroRecursion's intensive scenario work—millions of limbic comparisons across the five Fs of survival threat—functions as practice that reshapes the threat response networks. Just as motor learning produces refined movement control through repeated engagement, NeuroRecursion's repetitive survival-relevant comparisons produce refined threat assessment and neutralization of originally traumatic triggers through intensive limbic circuit reorganization.
Research Areas

Olivier Hardt
Neuroscientist, Memory Reconsolidation Researcher
Swiss Centre for Affective Sciences, University of Geneva
Department of Psychology and Neuroscience
Education
B.S. University of Geneva, Ph.D. University of Geneva
Research Focus
Emotional Memory and Reconsolidation-Based Therapy
Research
Olivier Hardt extended Nader's reconsolidation theory to show that emotional and fear memories—precisely what NeuroRecursion targets—are especially responsive to reconsolidation-based modification. His research demonstrates that even old, apparently stable trauma memories can be reactivated and updated if the right conditions create sufficient instability in the memory trace.
Hardt's key insight is that emotionally charged memories are not more resistant to modification but rather more susceptible to it—the very intensity that makes them intrusive also makes them malleable during reconsolidation. NeuroRecursion leverages this: by reactivating the trauma memory in the context of overwhelming, wildly absurd threat scenarios, Hardt's research predicts the memory becomes highly destabilized and maximally responsive to updating.
Hardt's demonstration that specific molecular events can be targeted therapeutically during reconsolidation provides the mechanism for NeuroRecursion's permanence: the intensive recursive scenarios don't just expose the person to the threat in imagination; they create optimal neurochemical conditions for reconsolidation-based updating—triggering protein synthesis and synaptic modification that literally rewrites the original memory trace. His work validates that even deeply entrenched emotional memories can be fundamentally modified through sufficiently intense, targeted engagement during the reconsolidation window.
Research Areas
Supportive Communities
The Neuro Recursion Institute supports the world's leading non-governmental organizations dedicated to neurodivergent advocacy, clinical research, and systemic support.
Contact us to suggest a partnership or collaboration.

WHO (World Health Organization) - Mental Health Division
The UN's primary health authority, with global programs in mental health, neurology, and disability prevention across 194 countries.
https://www.who.int/health-topics/mental-health
UNICEF (UN Children's Fund)
The world's largest organization dedicated to children's welfare, operating in 190 countries with programs for health, education, and protection.
https://www.unicef.org/
UNODC (UN Office on Drugs and Crime)
The UN agency fighting drug trafficking, crime, and corruption with programs for substance abuse prevention and treatment in 190+ countries.
https://www.unodc.org/
World Federation for Mental Health (WFMH)
A global organization advancing mental health advocacy, awareness, and promotion across 150+ countries with 320+ member organizations.
https://www.wfmh.global/
World Psychiatric Association (WPA)
The global federation of psychiatric societies representing 250,000+ psychiatrists and promoting mental health care in 140+ countries.
https://www.wpanet.org/
World Federation of Neurology (WFN)
The global federation of neurological societies providing education, research, and patient advocacy across 130+ countries.
https://www.wfneurology.org/
Médecins Sans Frontières (Doctors Without Borders)
An international humanitarian organization providing medical aid to people affected by conflict, disease, and disaster.
https://www.msf.org/
Amnesty International
A global human rights organization with 10+ million members advocating for justice and human dignity across 150+ countries.
https://www.amnesty.org/
Autism Speaks
The world's largest autism advocacy organization, focusing on research and global awareness.
https://www.autismspeaks.org/
PDA Society
The primary global organization defining and advocating for the PDA profile of autism.
https://www.pdasociety.org.uk/
CHADD (Children and Adults with ADHD)
The leading non-profit providing evidence-based training and advocacy for the ADHD community.
https://chadd.org/
International Dyslexia Association (IDA)
The oldest organization dedicated to the study and treatment of dyslexia worldwide.
https://dyslexiaida.org/
The Dyscalculia Association
Provides specialized research and teacher training for numerical processing disorders.
https://www.dyscalculia.me.uk/
Dysgraphia Support
An organization providing resources for writing disorder research and support.
https://www.dysgraphia.life/
Dyspraxia Foundation (UK)
The leading international resource for Developmental Coordination Disorder research and support.
https://dyspraxiafoundation.co.uk/
Dyspraxia USA
An organization dedicated to raising awareness and support for dyspraxia.
https://dyspraxiausa.org/
STAR Institute for Sensory Processing
The premier global center for SPD research, treatment, and education.
https://sensoryhealth.org/
National Stuttering Association (NSA)
The world's largest support organization for people who stutter.
https://westutter.org/
Stuttering Help (Also known as Speech Easy)
An organization providing facts, support, and resources for stuttering.
https://www.stutteringhelp.org/
Selective Mutism Association
An organization providing resources and support for selective mutism.
https://www.selectivemutism.org/
Learning Disabilities Association of America
An organization providing research and resources on learning disabilities.
https://ldaamerica.org/what-is-dyscalculia/
World Literacy Foundation
An international organization promoting literacy and education access globally, supporting reading and writing development for all ages.
https://worldliteracyfoundation.org/
ASHA (American Speech-Language-Hearing Association)
The leading organization for speech-language pathology and audiology professionals.
https://www.asha.org/
Brain and Spine Foundation (Global)
An international organization providing information and support for neurological and spinal conditions with research partnerships worldwide.
https://www.brainandspine.org.uk/
The Neurological Alliance
A UK-based alliance of organizations supporting people affected by neurological conditions.
https://www.neural.org.uk/
Epilepsy Foundation
A leading organization providing research, education, and support for epilepsy.
https://www.epilepsy.com/
Tourette Association of America (TAA)
The premier global entity for research into the CSTC loops and clinical support for tic disorders.
https://tourette.org/
International Association for the Study of Pain (IASP)
A global organization advancing pain research and clinical care.
https://www.iasp-pain.org/
American Migraine Foundation
A leading organization advancing migraine research and patient education worldwide.
https://americanmigrainefoundation.org/

TLC Foundation for Body-Focused Repetitive Behaviors (BFRB)
An organization providing support and research for hair pulling, skin picking, and nail biting disorders.
https://www.bfrb.org/
Anxiety and Depression Association of America (ADAA)
Focuses on the prevention and treatment of anxiety, phobias, and related disorders.
https://adaa.org/
Anxiety Canada
A Canadian organization providing evidence-based resources for anxiety disorders.
https://www.anxietycanada.com/

International OCD Foundation (IOCDF)
A global donor-supported organization dedicated to helping those with OCD and related disorders.
https://iocdf.org/
Depression and Bipolar Support Alliance (DBSA)
A peer-led organization providing support groups and clinical information for mood disorders.
https://www.dbsalliance.org/
International Bipolar Foundation (IBPF)
Focuses on global outreach and providing free resources to those living with bipolar disorder.
https://ibpf.org/
Bipolar UK
A leading UK organization providing information and support for bipolar disorder.
https://www.bipolaruk.org/
National Eating Disorders Association (NEDA)
A leading organization providing resources and support for eating disorders.
https://www.nationaleatingdisorders.org/
Alcoholics Anonymous (AA)
The world's largest peer-support organization for alcohol recovery, with millions of members in 180+ countries.
https://www.aa.org/
Narcotics Anonymous (NA)
A global fellowship for drug addiction recovery with individuals recovering in 140+ countries.
https://www.na.org/
Al-Anon
A global peer-support organization for families and friends of alcoholics.
https://www.al-anon.org/
World Federation Against Drugs (WFAD)
A multilateral umbrella organization for NGOs working on drug prevention and recovery.
https://www.wfad.se/
Addiction Center
A leading resource for substance abuse treatment and recovery information.
https://www.addictioncenter.com/
Find Treatment - SAMHSA
A US government resource for finding treatment for substance use and mental health.
https://findtreatment.gov/
Mind (UK Mental Health Charity)
A leading UK mental health organization providing information, support, and advocacy with international research partnerships.
https://www.mind.org.uk/
Mental Health America (MHA)
A comprehensive mental health organization providing screening, education, and advocacy across the United States.
https://www.mhanational.org/
Mental Health Foundation (Global)
An international charity advancing mental health research, awareness, and prevention across Europe and beyond.
https://www.mentalhealth.org.uk/
Hope + Me
Provides accessible mental health support and community resources for those in crisis.
https://www.hopeandme.org/
Gidget Foundation Australia
Supporting the mental health of new and expectant parents through evidence-based programs.
https://www.gidgetfoundation.org.au/
Psychology Today
A leading online resource for mental health information, therapist directory, and wellness articles.
https://www.psychologytoday.com/
Greater Good Science Center
A UC Berkeley center researching happiness, mindfulness, and social connection.
https://greatergood.berkeley.edu/
Campaign to End Loneliness
A UK coalition organization working to reduce loneliness and social isolation.
https://www.campaigntoendloneliness.org/
National Sleep Foundation
An organization advancing sleep health education and research.
https://www.thensf.org/
Impostor Syndrome Support
Resources and support for understanding and overcoming impostor syndrome.
https://impostorsyndrome.com/
NAMI (National Alliance on Mental Illness)
A grassroots mental health organization providing advocacy, education, support, and public awareness for those living with mental illness.
https://www.nami.org/
Postpartum Support International (PSI)
A global organization providing support for women experiencing perinatal mood and anxiety disorders.
https://www.postpartum.net/
Suicide & Crisis Lifeline
The nation's leading 24/7 suicide and crisis prevention organization.
https://suicidepreventionlifeline.org/
The Trevor Project
The leading suicide prevention and crisis intervention organization for LGBTQ+ young people.
https://www.thetrevorproject.org/
RAINN (Rape, Abuse & Incest National Network)
The nation's leading anti-sexual violence organization providing support and advocacy.
https://rainn.org/
The Hotline - Domestic Violence Support
The nation's leading domestic violence hotline providing 24/7 support.
https://www.thehotline.org/
VAWnet (Violence Against Women Network)
A resource network providing information on sexual abuse and domestic violence.
https://www.vawnet.org/
National Center for Trauma-Informed Care (NCTSN)
A center advancing trauma-informed approaches in mental health and healthcare systems.
https://www.nctsn.org/
National Center for PTSD (VA)
A US Veterans Affairs center providing PTSD research and treatment resources.
https://www.ptsd.va.gov/
Futures Without Violence
A global nonprofit organization working to prevent violence and trauma with evidence-based strategies.
https://www.futureswithoutviolence.org/
Gun Violence Archive
A research organization documenting gun violence incidents and providing accessible data on the human impact of gun violence.
https://www.gunviolencearchive.org/
One Love Foundation
Teaches young people to recognize and prevent unhealthy and abusive relationships.
https://www.joinonelove.org/
Mayo Clinic
A world-renowned medical center advancing healthcare research and patient care.
https://www.mayoclinic.org/
American Psychological Association (APA)
The world's largest professional psychology organization advancing psychological science and practice.
https://www.apa.org/
AASECT (American Association of Sexuality Educators, Counselors and Therapists)
A global organization advancing sexual health education and professional training.
https://www.aasect.org/
AAMFT (American Association for Marriage and Family Therapy)
The professional organization for marriage and family therapists advancing treatment and research.
https://www.aamft.org/
American Academy of Neurology (AAN)
The world's largest professional association of neurologists and neuroscience professionals advancing neurological care and research.
https://www.aan.com/
North American Menopause Society
An organization providing education and resources on menopause and hormone therapy.
https://www.menopause.org/
National Institute on Aging (NIA)
A US government agency researching aging, dementia, and age-related health conditions.
https://www.nia.nih.gov/
HospiceNet
An organization providing information and resources about end-of-life care.
https://www.hospicenet.org/
NAACP (National Association for the Advancement of Colored People)
America's oldest and largest civil rights organization dedicated to racial equality and social justice.
https://www.naacp.org/
Anti-Defamation League (ADL)
An international organization fighting discrimination and promoting civil rights.
https://www.adl.org/
Ceasefire Now
An international organization advocating for conflict prevention and peace-building initiatives.
https://www.ceasefirenow.org/
HelpAge International
The leading global organization dedicated to improving the lives of older people in poor countries.
https://www.helpage.org/
SOS Children's Villages
A global humanitarian organization supporting vulnerable children and families.
https://www.sos-childrensvillages.org/
Zero to Three
A global organization focused on infant and early childhood development.
https://www.zerotothree.org/
JA Worldwide (Junior Achievement)
A global social enterprise providing entrepreneurship and financial literacy education to youth.
https://www.jaworldwide.org/
National Foundation for Youth Improvement
An organization supporting youth development and mental health programs.
https://www.nfyi.org/
CODA (Children of Deaf Adults)
A support organization for children of deaf parents.
https://www.coda.org/
National Stepfamily Resource Center
Resources and research for stepfamilies and blended families.
https://www.stepfamilies.info/
World Council for Gifted and Talented Children (WCGTC)
A worldwide network that supports research and educational policies for gifted individuals.
https://world-gifted.org/
International Cultic Studies Association (ICSA)
A global nonprofit organization advancing education and research on psychological manipulation, undue influence, and coercive control.
https://internationalculticstudies.org/